


Introduction
Chest tube placement (also called tube thoracostomy) is a common procedure in daily clinical practice which is performed to drain fluid, blood, or air from the pleural cavity. It also serves as a route to instill antibiotics (post-pneumonectomy empyemas), sclerosing agents (pleurodesis), as well as fibrinolytics, DNAse, and/or saline (complicated parapneumonic effusions and empyemas). On the other hand, indwelling pleural catheters (IPC) are becoming a first-line palliative therapy for symptomatic malignant and persistent benign pleural effusions.
A recent expert consensus has stated that interventional pulmonology fellowships in the United States should perform a minimum of 20 each image-guided thoracostomy and IPC placement procedures annually for standard accreditation1. Consequently, pulmonologists should be familiar with the main indications, contraindications, technical aspects, and complications of inserting a chest tube in the pleural space; all of which will be succinctly addressed in the present review.
Indications and Contraindications of Chest Tube Placement
Indications for the insertion of an intercostal chest drain are listed in Table 1. The most common include pneumothoraces, complicated parapneumonic effusions or empyemas, hemothoraces, bedside pleurodesis, and following cardio-thoracic surgery or thoracoscopic procedures to allow for appropriate lung re-expansion2. Moreover, IPC provide symptomatic relief in patients with large malignant effusions, benign effusions resistant to medical therapies, effusions which failed following an attempted pleurodesis, and effusions associated with unexpandable lungs2.
The only absolute contraindication for tube thoracostomy is the lack of informed consent or patient cooperation. Relative contraindications include uncorrected coagulopathy (e.g., patients with international normalized ratio >1.5-2 or with a platelet count <50,000/µL) and instrumental access to the pleural cavity without image-guidance in patients with substantial pleuro-pulmonary adhesions or multiloculations3,4. Chest tube insertion over an infected skin area should be avoided.
Chest Tube Types and Sizes
There are many kinds of chest tubes or catheters, but they are basically classified according to size and method of insertion5. Commercially available chest tubes are made of different materials, including polyvinyl chloride, polyethylene, and silicone. They can be straight, angled, or coiled at the end (“pig-tail”). They contain a number of holes along the side and the tip, and all have a radiopaque stripe with a gap that serves to mark the most proximal drainage hole (“sentinel” hole). Some tubes have a double lumen, the small one normally being used for irrigation.
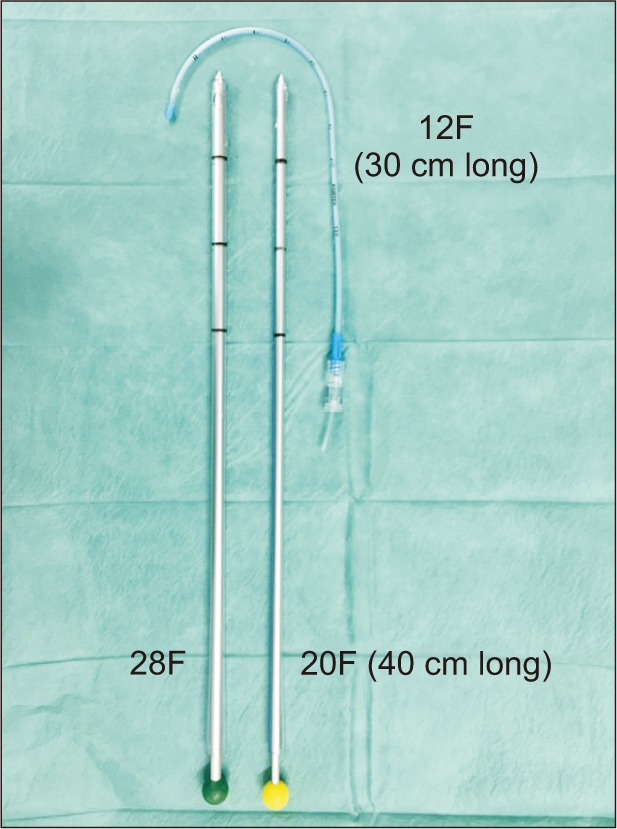
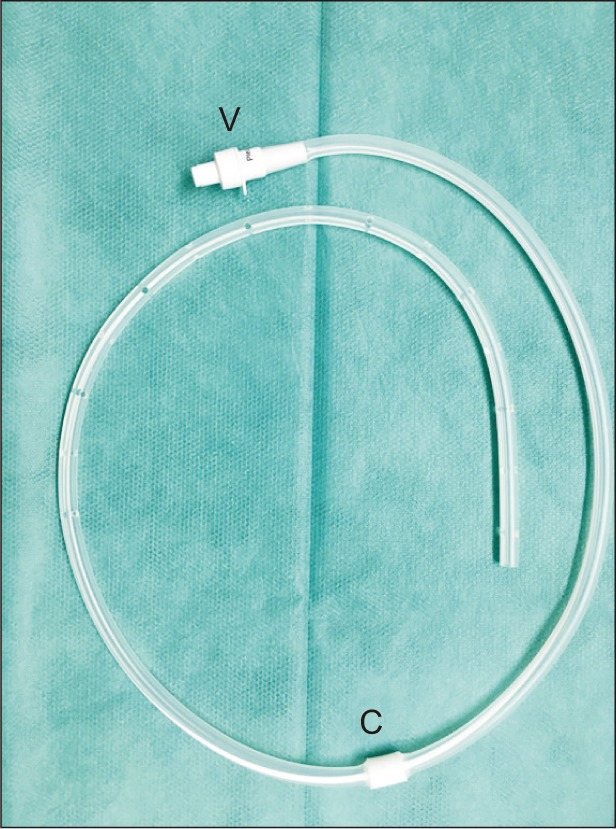
The internal diameter and length of chest tubes determine the air or liquid flow rate through the drain, according to the Poiseuille's law (liquids) and the Fanning equation (gases)6. The size of a chest tube refers to its outer diameter and is given in “French” (F) or “Charrière” (Ch), with 1F corresponding to one-third millimeter. Thus, a 12F tube is 4 mm in diameter. Chest tube sizes usually range between 8F and 36F (Figure 1). A general distinction is made between small-bore chest tube (SBCT) and large-bore chest tube (LBCT), but the threshold size to establish this categorization is being set at either 14F or 20F7,8. For the purpose of this review, SBCT are defined as 14F or less, and LBCT as greater than 14F, unless otherwise indicated. Within this categorization, some authors also prefer to consider a group of medium-bore tubes (16-24F)2,3. IPC is a fenestrated silicone 15.5F catheter, 66 cm in length with side holes over the distal 24 cm, which is tunneled to prevent dislodgment and infection (Figure 2).
The optimal chest tube size for the management of pleural diseases is still a matter of debate. The British Thoracic Society guidelines suggest that in pneumothoraces and effusions of a malignant or an infectious nature (including empyemas) SBCT are usually adequate9,10,11, although there is a lack of randomized trial data. However, the Therapeutic Interventions in Malignant Effusion (TIME1) randomized controlled trial found that 12F chest tubes were associated with a higher pleurodesis failure than 24F chest tubes (30% vs. 24%) in 100 patients with malignant effusions, suggesting that chest tube size matters for pleurodesis efficacy12. Moreover, even though the smaller chest tubes resulted in significantly less pain than the larger ones, the difference was not likely clinically significant (mean visual analog scale of 22 vs. 26.8)12. Based upon expert opinion, use of chest tubes ≥20F is recommended in the following situations2,3,5,13: (1) there is clinical concern for the presence of an on-going air leak (or significant risk of it, as in traumatic pneumothorax or bronchial dehiscence), (2) iatrogenic pneumothorax from barotrauma (mechanical ventilation), (3) hemothoraces, and (4) postoperative drainage of the chest cavity.
Techniques for Chest Tube Placement
SBCT and medium-bore chest tubes are typically placed using the Seldinger technique, whereas LBCT (>24F) can be inserted by blunt dissection or the trocar technique. The Seldinger technique has become the most widespread method of tube placement because of the ease of insertion and increased patient comfort14. Conversely, the trocar technique is obsolete and should never be employed since it significantly increases the risk of misplaced drains and organ perforation15.
The insertion of a chest tube can be performed at the bedside or the endoscopic suite for most patients, with the exception of those which are placed after cardio-thoracic surgery. A single chest tube is sufficient for most drainage indications, but occasionally two simultaneous or consecutive tubes may be necessary for the effective drainage of non-communicating infected fluid collections following a trial of intrapleural fibrinolytics.
1. Preparation, patient positioning, and local anesthesia
After an explanation of the advantages and possible complications of the procedure, patients should give written informed consent, except in emergency situations. A recent chest radiograph should be available to the operator. The administration of prophylactic antibiotics prior to chest tube placement (e.g., a single dose of cefazolin 2 g intravenously) is only recommended in patients with penetrating chest injuries16. In addition to local anesthesia, conscious sedation with an opioid (e.g., 2.5 mg morphine intravenously, fentanyl) or benzodiazepine (e.g., 1-2 mg midazolam intravenously) might be considered when inserting LBCT in anxious patients who are hemodynamically stable5,17.
The first step involves positioning the patient according to the location chosen for drain insertion. Ideally, chest tubes should be inserted at the 4th-5th intercostal space in the anterior or mid-axillary line. To access this area, the patient is positioned supine, lying on the bed at 45°-60°, slightly rotated, and with the ipsilateral arm behind the neck or over the head14,17. The lateral decubitus position with the affected hemithorax upmost is also possible, but many times it is not tolerated by patients with massive pleural effusions. If the patient has a posterior loculated fluid collection (e.g., empyema), he/she will be in a seated position with the physician standing behind. Finally, in patients with pneumothorax, the second intercostal space in the mid-clavicular line (Monaldi position) has long been suggested as an alternative site5. However, it is not the best choice because the incision is in a very visible location with the potential for leaving an unsightly scar, the intercostal space is narrow in this site, and it requires penetrating the pectoralis muscle. Consequently, only if very thin catheters (8F) are used can this insertion point be considered an acceptable option, particularly in apical or anterior pneumothoraces.
Bedside ultrasound (US) should be used to mark the entry point for all chest tubes in patients with pleural effusions in order to prevent incorrect placement and reduce risk of accidental organ injury associated with the procedure18. It is common to insert the drain using the so-called free-hand technique, where the physician marks the entry point under US guidance and the procedure is performed immediately thereafter while the patient remains motionless. Procedures where the radiologist marks the puncture location and the physician performs the tube thoracotomy procedure at a later point (“X marks the spot” technique) are highly discouraged, since it is nearly impossible for the patient to assume the same position they were in when being marked18. Real-time imaging, using US or computed tomography, may be necessary when inserting drains into small or anatomically difficult-to-access effusions. Experienced US operators may detect vulnerable intercostal vessels using a linear probe, thus avoiding accidental puncture of an intercostal artery.
Chest tube insertion is a full aseptic technique; therefore, sterile gloves, gowns, surgical mask, and drapes should be used. Skin disinfection with 10% povidone-iodine or 2% chlorhexidine solutions is confined to the target area, and swabbing from the point of insertion outwardly in a circular motion is recommended17. Once sterile drapes are arranged, local anesthetic infiltration of the skin, subcutaneous tissue (25G needle) and parietal pleura (21G needle) with 1% or 2% mepivacaine (or alternatively, 1% or 2% lidocaine) should be performed. When air or fluid is aspirated, the needle is withdrawn until it ceases; then, further local anesthetic is injected, thus allowing an effective infiltration of the parietal pleura. Importantly, a previous history of allergy or hypersensitivity reactions to local anesthetics should be recorded before their administration. Moreover, not infrequently an excessive quantity of local anesthetic produces transitory central nervous system (e.g., drowsiness, confusion, convulsions, focal neurological findings)19 and cardiovascular toxicities (e.g., hypotension, arrhythmias). Total infiltration of up to 20 mL of 2% mepivacaine or 2% lidocaine is admissible.
A detailed stepwise description of the techniques for chest tube insertion is beyond the scope of this article. Regardless of the adopted techniques, the tube must be placed on the superior rib margin to avoid injury to the intercostal neuromuscular bundle.
2. Small-bore chest tubes (Seldinger technique)
SBCT are commonly placed using the catheter-over-guide wire (Seldinger) technique, in which a guide wire is inserted into the pleural space through an introducer needle; the wire should pass without resistance. Then, the needle is removed and dilators are threaded over the wire using a slight twisting action. Afterwards, the chest tube is threaded over the guide wire and into the pleural space, where remains14,17. In cases of pneumothorax, SBCT are directed toward the apex, but for pleural effusions they are directed both inferiorly and posteriorly into the diaphragmatic recess. A silk or synthetic monofilament suture (number 1) along with an adhesive dressing secure the tube in position. An attached 3-way stopcock connects the tube with the drainage system. A chest radiography to confirm the chest tube position is mandatory.
Advantages of SBCT include the need for a small incision (resulting in minimal scarring), less painful insertion, and better tolerability by the patient. However, lumen blockage is a concern, making it advisable to flush 20 mL of saline every 8-12 hours as a preventative20.
3. Large-bore chest tubes (blunt dissection technique)
Blunt dissection is the standard technique for inserting LBCT. It requires an incision of the skin and subcutaneous tissue large enough to allow the introduction of a finger into the pleural space in order to avoid or break down pleuro-pulmonary adhesions and ensure proper chest tube positioning17,20. Before finger insertion, an artery forceps or Kelly clamp must be used to bluntly dissect the intercostal tissues. The skin incision should be made a couple of centimeters below the upper rib edge through which the pleural space will be accessed, thus permitting the creation of a tunnel of subcutaneous tissue which helps to prevent air re-entry once the tube is removed (coulisse effect)5. The chest tube should be held in place using heavy suture material (silk number 0 or 1). An additional “U-stitch” is commonly placed around the tube, and tied to close the wound after the tube is removed. As for SBCT, a chest radiograph should be obtained to check for proper positioning, except chest tubes placed post-operatively. The sentinel hole should be at least 2 cm beyond the rib margin. Although LBCT are less susceptible to clogging or kinking than SBCT, they represent a more invasive approach.
4. Indwelling pleural catheters
IPC insertion entails the subcutaneous tunneling of the catheter between two incisions (about 5 cm apart). A polyester cuff is placed half way along this tunneled part and acts as a barrier to infection and promotes adhesion to the subcutaneous tissue to secure the catheter in place (Figure 2). The pleural space is accessed using the Seldinger technique with a Teflon “peel-away” dilator. With the fenestrated portion of the catheter inside the thoracic cavity, the external portion contains a one-way valve that allows fluid and air to go out, but not in, once attached to a vacuum bottle21. There are three IPC manufacturers: PleurX (CareFusion) which continues to be the industry standard, Rocket IPC Pleural Catheter, and Aspira Pleural Drainage System (Bard).
The procedure is usually performed in an ambulatory, day care setting, unless the patient has already been admitted for another reason22. It is recommended to prescribe adequate analgesia (e.g., acetaminophen plus a weak opioid) for at least two weeks following the IPC placement23. Intermittent pleural fluid drainage is done at home by a trained family member or a healthcare provider.
Chest Drainage Systems
Once a chest tube is in place, a chest drainage system (CDS) is attached. There are basically four types of CDS: one-way Heimlich valve, analog three-container systems, digital or electronic CDS, and simple vacuum bottles (for IPC drainage)5.
1. Heimlich valve
The one-way Heimlich valve is a simple device which contains a rubber flutter valve that is occluded during inspiration (negative intrapleural and intratube pressure), thus preventing air from entering the pleural space; while being held open during expiration (positive pleural pressure) allowing the egress of air or fluid from the pleural space (Figure 3). Heimlich valves are used for the ambulatory management of pneumothorax (including patients with persistent air leaks) or tension pneumothoraces24. There are commercially available 8F catheters coupled with a self contained one-way valve and vent, which allows full patient mobility during treatment of pneumothorax (e.g., Rocket Pleural Vent).
2. Three-compartment chest drainage systems
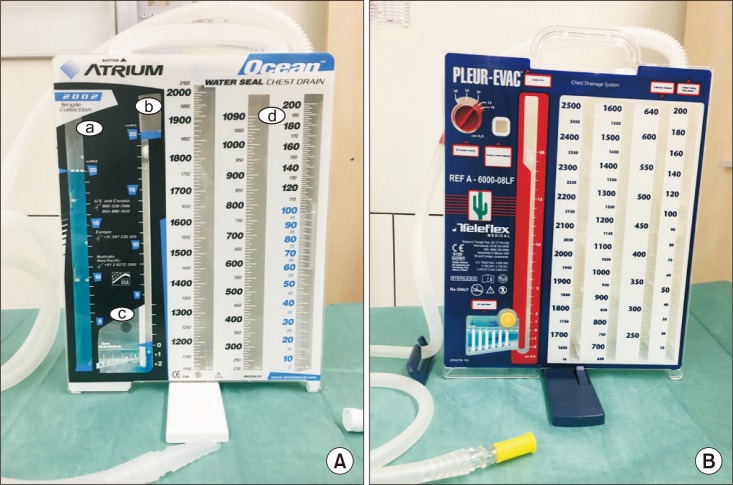
Three-chamber plastic units (e.g., Pleur-evac, Atrium) are probably the most commonly used CDS25. They include a collection chamber, a water-seal chamber and a suction control chamber, which are interconnected. Fluid or air drain into the collection chamber. The water-seal chamber holds a column of water (2 cm) which prevents air from being sucked into the pleural space with inspiration. Finally, the suction chamber may use a wet (water column) or a dry (valve regulator) suction mechanism that allows the suction level to be adjusted for up to −40 cm H2O for the dry device versus a maximum of −25 cm for water columns; −20 cm H2O being the typical initial pre-set level (Figure 4). This suction chamber can be attached to continuous wall (external) suction to remove air or fluid, or it can be placed on “water seal” with no active suction mechanism (gravity drainage).
Intermittent or constant bubbling within the water-seal chamber is indicative of an air leak, which is often more apparent when the patient coughs. Causes of bubbling other than a visceral pleural tear include a migrated tube with drainage holes outside the skin, or an inadequate closure of the chest tube insertion site. Moreover, patency of the chest tube is verified by observing respiratory fluctuations of the fluid in the water-seal chamber when the patient is on gravity drainage; no fluctuation indicates that either the tube is occluded or the lung is completely expanded and has blocked the holes of the chest tube inside the chest cavity. Swinging of the fluid in the collecting tube during respiratory cycles (“tiding”) is also characteristic of a correctly placed chest tube.
Whether to apply “suction or no suction” (with “suction” meaning external suction, and “no suction” meaning water seal) is a decision to be made individually6. It is prudent to start with water seal in patients with pneumothoraces, pleural effusions, or following lung resection surgery (not lung reduction surgery or pneumonectomy). Only if an air leak persists or the lung does not completely re-expand should suction be applied. When using water seal (as opposed to digital drainage systems), it is mandatory to keep the canister positioned below the chest.
In the case of massive pleural effusions, the initial drainage should be controlled to prevent re-expansion pulmonary edema. It is necessary to clamp the tube if the patient develops respiratory symptoms (i.e., coughing, chest tightness or pain, shortness of breath or oxygen desaturation) or recommended after draining 1.5 L26. Drainage may be interrupted for up to one hour or more, or until symptoms resolve, and then resumed.
3. Digital drainage systems
Digital drainage systems (e.g., Thopaz, Medela; Atmos; Dentrex, Redax) are gradually becoming used in pneumothoraces and following thoracic surgery (Figure 5). These devices reduce inter-observer variability in air leak assessment since they provide a continuous digital recording of air leak, fluid drainage and intrapleural pressure5,27. They maintain a predetermined intrathoracic pressure (usually −8 cm H2O), and the system intervenes only as needed to achieve the desired value. Digital systems give the patient the freedom to ambulate without being attached to wall suction. Overall, these electronic systems contribute to shortening hospital stay by leading to earlier chest tube removal. Moreover, patients can be discharged with these devices in place, if necessary.
4. Vacuum bottles
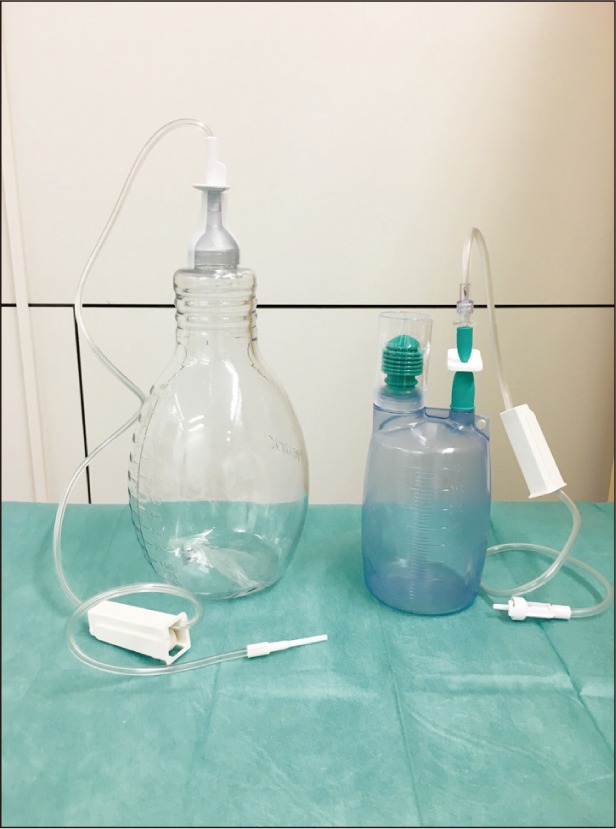
Drainage of pleural fluid through an IPC is performed by connecting the external one-way valve to a vacuum bottle. The latter is supplied by the IPC manufacturer (1 L capacity) or, alternatively, Redon disposable drainage vacuum bottles (200, 400, and 600 mL capacity) may be employed (Figure 6). Instead of using vacuum bottles for pleural drainage, the Aspira catheter uses a manual pump, which is attached to the catheter and a collection bag in line28. The patient squeezes the pump to initiate the vacuum effect and the fluid drains into the collection bag.
The first drainage session should generally avoid removal of more than 1.5 L (or less if drainage causes chest pain or cough secondary to unexpandable lung), as detailed previously. Thereafter, there are no data to guide optimal drainage frequency26. It usually varies from once daily to 2 to 3 times weekly or may even be tailored to the patient's symptoms. A recently completed randomized controlled trial favored daily over alternate IPC drainage in that it led to a higher rate of spontaneous pleurodesis (47% vs. 24%) in a shorter period (54 vs. 90 days)29.
Chest Tube Removal
Most chest tubes are suitable for leaving inside the pleural space for more than 2 weeks. However, the longer the tube remains, the greater the risk of local infectious complications. On the other hand, aspiration drain systems designed for therapeutic thoracenteses (8F), which may occasionally be used for draining small empyematous collections, are usually made of polyurethane and should be removed no later than three days after their initial insertion5.
Chest tubes are withdrawn when they reach their predefined therapeutic goals or become nonfunctional. In patients with pneumothoraces or following thoracic surgery, a clamping trial and a chest radiograph are unnecessary prior to removal of tube thoracostomy to detect recurrent pneumothorax, provided a digital recording drainage device shows that the patient has no air leaks30. Acceptable air flows for chest tube removal are below 20 mL/min for 8-12 hours when no suction is applied, or less than 40 mL/min for 6 hours in accordance with other authors5,31. However, when conventional analogue pleural drainage devices are employed, the chest tube is pulled out if the lung remains fully expanded on a chest radiograph performed off suction, and no air bubbling in the water seal chamber is observed. A bubbling chest tube should never be clamped, since this may lead to tension pneumothorax. If doubts on the presence of an air leak exist, some clinicians prefer to perform a clamp trial, a risky maneuver that requires close monitoring of the patient and generally leads to unneeded delay of chest tube removal5.
In cases of pleural effusion, the fluid output threshold for chest drain removal is not standardized and depends on the underlying disease. In postoperative situations, chest tubes can be safely withdrawn with daily outputs up to 450 mL/24 hr31. Following pleurodesis, some pulmonologists remove the drain when fluid production is below 100-150 mL/day while others do it at a specific time (e.g., 24 hours) after the instillation of the sclerosing agent, regardless of fluid volume output32.
In preparation for removal, the tube should be taken off suction, placed on water seal and removed quickly at the end of expiration during a Valsalva maneuver while placing a sterile dressing over the insertion site31. After suturing the opening, an occlusive dressing with povidone-iodine is applied to the wound.
In IPC patients, when the pleural fluid output drops to less than 50 mL on three consecutive drainages, spontaneous pleurodesis is assumed21, provided a bedside US rules out the presence of pleural fluid (i.e., the declined drainage cannot be attributed to catheter blockage). In these circumstances the pleural catheter may be removed. Spontaneous pleurodesis occurs in about 50% of patients26. For IPC withdrawal, the adhesions surrounding the cuff need to be freed, usually with a metallic groove director.
Complications
The average rate of complications during or following placement of a chest tube is less than 10% (Table 2), and mainly depends on operator experience, the size of the tube and use of imaging to guide insertion33,34,35. Fewer complications appear when experienced operators insert SBCT under image guidance. In a British audit of 58 hospitals, 824 chest drain procedures were evaluated, of which 83% corresponded to SBCT, 80% made use of the Seldinger technique, and about half were performed under real-time US36. The most frequent immediate complications were pain (4.1%), failure to place the drain (2.4%) and vasovagal reactions (2.1%), while delayed complications included pain (18%), drain blockage (7.4%), accidental dislodgment (7.3%), and subcutaneous emphysema (3.4%)36. As far as LBCT (≥20F) is concerned, commonly reported post-insertion complications are malposition (6.5%), drain blockage (5.2%), organ injuries (1.4%), and empyema (1.4%)20.
Chest tube malpositions can be classified as intrafissural, intraparenchymal, and subcutaneous. They should be initially suspected if the chest tube is not draining, and are supported by chest radiographic findings. But often, a computed tomography is necessary to better assess malpositioned tubes. In cases of intraparenchymal misplacement, a second functioning chest tube should be placed prior to the removal of the original to avoid tension pneumothorax or extensive subcutaneous emphysema34. Rather than being reintroduced, any dislodged nonfunctional tube should be replaced, due to the risk of infection associated with the reinsertion of the externalized portion of the tube.
Hemothorax may result from intercostal artery laceration or, less commonly, from injury to vascularized pleural tumors. Although this complication is usually evident during or after the procedure, sometimes bleeding remains undetected due to the tamponade effect of the chest tube itself until the drain is removed33,34.
Subcutaneous emphysema involving chest wall, neck, and face presents as a subcutaneous crepitation, and is easily detectable on chest radiographs. Fortunately, it is usually a minor and self-limiting complication. Tube blockade or migration of the sentinel hole out of the pleural space should be checked. This complication may need tube thoracostomy replacement and even subcutaneous incisions or drains.
Complications associated with IPC use occur in 10%-20% of patients26. Many are common for any chest tube drain, as referred to above, though others are more specific to this procedure. IPC blockage and symptomatic loculations (i.e., a multiseptated effusion which fails to evacuate through a patent IPC) may require intrapleural fibrinolysis. IPC-related infection develops in about 5% of the cases and remains the strongest concern26. However, the infections are generally mild and can often be managed conservatively (e.g., antibiotics, saline lavage, drainage of the infected material through the IPC), without needing immediate IPC removal.
Conclusion
Tube thoracostomy is a procedure which can be performed by trained pulmonologists. Other than postoperative chest tubes, most procedures consist of the US-guided insertion of SBCT with the Seldinger technique in patients with pneumothoraces, complicated parapneumonic effusions/empyemas, or malignant pleural effusions. Hemothoraces usually require LBCT, which can be placed by Seldinger or blunt dissection techniques. Detection of air leaks in patients with pneumothoraces or following thoracic surgery has been greatly improved with the use of electronic CDS. Finally, IPC are becoming a first-line therapy of symptomatic malignant and persistent benign pleural effusions. They are commonly placed as a day case and allow long-term intermittent fluid drainage in the outpatient setting. Pulmonologists should be familiar with the common complications that may occur during or after chest tube insertion, some of which are potentially dangerous (e.g., malposition, hemothorax, infection, organ injury, or reexpansion pulmonary edema).


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






