Characteristics, Management, and Clinical Outcomes of Patients with Hospital-Acquired and Ventilator-Associated Pneumonia: A Multicenter Cohort Study in Korea
Article information
 , Kyung Hoon Min, M.D., Ph.D.2,*, Sang-Bum Hong, M.D., Ph.D.3, Ae-Rin Baek, M.D., Ph.D.4, Hyun-Kyung Lee, M.D., Ph.D.5, Woo Hyun Cho, M.D., Ph.D.6, Changhwan Kim, M.D., Ph.D.7, Youjin Chang, M.D., Ph.D.8, Sung-Soon Lee, M.D., Ph.D.9, Jee Youn Oh, M.D., Ph.D.2, Heung Bum Lee, M.D., Ph.D.10, Soohyun Bae, M.D., Ph.D.11,†, Jae Young Moon, M.D., Ph.D.12,‡, Kwang Ha Yoo, M.D., Ph.D.13, Kyeongman Jeon, M.D., Ph.D.1,14
, Kyung Hoon Min, M.D., Ph.D.2,*, Sang-Bum Hong, M.D., Ph.D.3, Ae-Rin Baek, M.D., Ph.D.4, Hyun-Kyung Lee, M.D., Ph.D.5, Woo Hyun Cho, M.D., Ph.D.6, Changhwan Kim, M.D., Ph.D.7, Youjin Chang, M.D., Ph.D.8, Sung-Soon Lee, M.D., Ph.D.9, Jee Youn Oh, M.D., Ph.D.2, Heung Bum Lee, M.D., Ph.D.10, Soohyun Bae, M.D., Ph.D.11,†, Jae Young Moon, M.D., Ph.D.12,‡, Kwang Ha Yoo, M.D., Ph.D.13, Kyeongman Jeon, M.D., Ph.D.1,14
Abstract
Background
Hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP) are significant public health issues in the world, but the epidemiological data pertaining to HAP/VAP is limited in Korea. The objective of this study was to investigate the characteristics, management, and clinical outcomes of HAP/VAP in Korea.
Methods
This study is a multicenter retrospective cohort study. In total, 206,372 adult patients, who were hospitalized at one of the 13 participating tertiary hospitals in Korea, were screened for eligibility during the six-month study period. Among them, we included patients who were diagnosed with HAP/VAP based on the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) definition for HAP/VAP.
Results
Using the IDSA/ATS diagnostic criteria, 526 patients were identified as HAP/VAP patients. Among them, 27.9% were diagnosed at the intensive care unit (ICU). The cohort of patients had a median age of 71.0 (range from 62.0 to 79.0) years. Most of the patients had a high risk of aspiration (63.3%). The pathogen involved was identified in 211 patients (40.1%). Furthermore, multidrug resistant (MDR) pathogens were isolated in 138 patients; the most common MDR pathogen was Acinetobacter baumannii. During hospitalization, 107 patients with HAP (28.2%) had to be admitted to the ICU for additional care. The hospital mortality rate was 28.1% in the cohort of this study. Among the 378 patients who survived, 54.2% were discharged and sent back home, while 45.8% were transferred to other hospitals or facilities.
Conclusion
This study found that the prevalence of HAP/VAP in adult hospitalized patients in Korea was 2.54/1,000 patients. In tertiary hospitals in Korea, patients with HAP/VAP were elderly and had a risk of aspiration, so they were often referred to step-down centers.
Introduction
Hospital-acquired pneumonia (HAP) is defined as the development of parenchymal lung infection in hospitalized patients after at least 48-hour post-admission. However, if patients who experience intubation to receive mechanical ventilation (MV) in an intensive care unit (ICU) and then these patients develop parenchymal lung infection within 48 hours of admission, the condition is known as ventilator-associated pneumonia (VAP)1. Furthermore, HAP/VAP is the most common nosocomial infection that causes significant clinical and economic burden, including prolonged hospitalization, higher overall health care costs, and increased morbidity and mortality 2–7. Previous epidemiological studies have been carried out at a worldwide level. These studies have reported the prevalence of HAP as 5–20 cases per 1,000 hospital admissions and 2.4–6.1 cases per 1,000 non-ICU patients6–11. However, the epidemiological data of HAP remains limited in Korea.
Several international organizations have provided guidelines for the appropriate management of HAP/VAP in patients 2,3. According to these guidelines, physicians should provide an empirical treatment only after considering the local epidemiological findings, etiology, and resistance patterns.
Epidemiological and microbiological information is very important in the management of HAP/VAP, but hospitals in Korea have published very little data about HAP/VAP patients. Therefore, in this study, we investigated the prevalence and underlying characteristics of HAP/VAP in Korean hospitals, which included microbiological information, epidemiology, and the outcomes of HAP/VAP in Korea.
Materials and Methods
1. Study design and population
A nationwide, multicenter retrospective cohort study was conducted by the Korean HAP/VAP Study Group. In this study, 13 tertiary or university-affiliated hospitals of Korea participated. The study protocol was developed by the steering committee, which periodically reviewed the progress of the study and provided an overall supervision of the research study. The study was approved by the institutional review boards of each participating hospital and Samsung Medical Center (No. 2020-03-150). They waived the compulsion of getting an informed consent letter as it was an observational study. In addition, patient information was anonymized and eliminated from records or files prior to analysis.
In this study, the inclusion criteria of patients was follows: (1) they were admitted to the participating hospital for more than three days (from June 1 to December 31, 2019), (2) they were labeled as pneumonia-related International Classification of Diseases-10 code (J13–J18, J85) at discharge, and (3) they were at least 19 years of age. All these patients were screened for eligibility. After performing a comprehensive review of medical records, patients were diagnosed with HAP/VAP based on the definition1 provided by the following organizations: the American Thoracic Society and the Infectious Diseases Society of America (HAP/VAP is a condition that includes new or progressive parenchymal lung infiltrate and clinical findings that suggest infection, e.g., the new onset of fever, purulent sputum, leukocytosis, and a decline in oxygenation). Such patients were included in the study and followed up until their date of death or hospital discharge. In this study, the exclusion criteria of patients was as follows: patients who had received antibiotics for more than 72 hours at other hospitals or who had developed pneumonia within 48 h of their transfer to another hospital.
2. Data collection
In each participating hospital, the trained study coordinators reviewed the electronic medical records of each patient, and they collected the data by using a standardized case report form. The information collected was as follows: (1) the demographic data, including age, sex, comorbidities, and clinical frailty score; (2) the data on HAP/VAP, including risk factors, disease severity, Sequential Organ Failure Assessment (SOFA) scores, laboratory variables, infectious pathogens, and multidrug resistant (MDR) pathogens; (3) the treatment data, including the adequacy of an empirical antibiotic therapy, the adjunctive use of steroids, ICU admissions, and limitations of care decision; and (4) clinical outcomes, including clinical and microbiological responses, in-hospital mortality, and the discharge destination of patients who survived and were discharged. In case of patients admitted to the ICU for HAP/VAP, the study coordinators also collected data pertaining to the use of resources and the occurrence of medical events during their stay in the ICU. All the participating hospitals were asked to complete data entries and email the data to the coordination center, where the quality of the data was assessed for completeness and for logical errors.
3. Definitions
An infection can be classified into three categories: (1) microbiologically documented infections, (2) clinically documented infections, and (3) possible infections. Cultured pathogens are defined as the microorganisms collected within 2 days of antibiotic treatment by the managing physicians; however, these microorganisms should not be colonizers or contaminants. Furthermore, MDR pathogens are defined as the microorganisms that are resistant to agents of three or more antimicrobial categories12. An initial antimicrobial therapy was provided in the absence of microbiological isolates, and was considered to be an empirical therapy. Based on the results of drug susceptibility testing, we gauged the adequacy of this empirical therapy. The baseline SOFA score was assumed to be zero in patients who did not have a pre-existing organ dysfunction13,14. The risks of aspiration were classified as follows: (1) an impaired swallowing (esophageal disease, neurological disease, or recent extubation), (2) an impaired consciousness, (3) an increased chance of gastric contents reaching the lung (reflux or tube feeding), and (4) an impaired cough reflex (medications, stroke, or dementia)15. Sepsis and septic shock were defined by the clinical criteria presented in the 3rd International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)16.
Clinical responses were classified according to the following three categories: (1) clinical cure (an improvement in all the signs and symptoms of pneumonia), (2) clinical failure (the persistence or worsening of signs, symptoms, or both of pneumonia; the symptoms or signs of pneumonia, or both, occurred within 3 days after the termination of medical treatment), and (3) the recurrence of pneumonia (the occurrence of a new event of pneumonia 72 hours after the discontinuation of antibiotics). In addition, microbiological responses were classified as follows: (1) microbiological eradication: an absence of the baseline pathogen in the final culture of specimens during hospitalization, (2) colonization: persistence of the baseline pathogen but clinically cured, (3) microbiological failure: persistence of the baseline pathogen with clinical failure, and (4) microbiological recurrence: regrowth of the baseline pathogen irrespective of the clinical outcome.
Results
1. Study population
The study was conducted for a period of 6 months, which extended from June 1 to December 31, 2019. During this period, 206,372 adult patients were admitted into the participating hospitals; however, only 526 patients were diagnosed with HAP/VAP (2.54/1,000 patients). Table 1 enlists the baseline characteristics of these patients: there were 360 male patients (68.4%), and 166 female patients (31.6%) with HAP/VAP; the median age of these patients was 71.0 years (range, 62.0–79.0 years). The most common comorbidities were as follows: solid malignant tumors (35.9%), diabetes (31.7%), and chronic neurological disease (27.9%). The median Charlson Comorbidity Index was 5.0 (3.0–6.0) and the Clinical Frailty Scale was 5.0 (3.0–7.0). The most common reasons for hospitalization were treatment of medical diseases (n=303, 57.6%), followed by elective operation (n=106, 20.2%).

Baseline characteristics of patients with hospital-acquired and ventilator-associated pneumonia
2. Clinical characteristics on the day of HAP/VAP diagnosis
In this study, HAP was diagnosed in 419 patients (79.7%) (379 patients in general ward and 40 patients in the ICU), whereas VAP was diagnosed in 107 (20.3%) patients (Table 2). Among the 526 patients, 381 patients (71.4%) were administered intravenous antibiotics for 90 days, and 149 patients (28.3%) were provided with artificial airways. A vast majority of patients (n=333, 63.3%) had at least one aspiration risk: the most common risk was impaired swallowing (n=223, 42.4%), followed by cases having an increased likelihood of retrograde gastric content flow to the lung (n=202, 38.4%). The median SOFA score was 4.0 (2.0–7.0). Sepsis was observed in 336 (63.9%) of the total patients, and septic shock was observed in 56 patients (10.6%).

Clinical characteristics on the day of diagnosis of hospital-acquired and ventilator-associated pneumonia
3. Diagnostic materials and microbiology
During the evaluation of pathogens, we found the highest number of analyzed specimens in blood cultures (79.3%), sputum (54.6%), and transtracheal aspirations (31.9%). Moreover, 99 patients (18.8%) had colonized pathogens before being diagnosed with HAP/VAP. The median value of C-reactive protein was 10.4 mg/dL (range, 6.1–17.9 mg/dL), and the median value of procalcitonin was 0.4 mmol/L (range, 0.4–0.4 mmol/L), respectively.
The pathogen involved was identified in 211 patients (40.1%) (Table 3). The most common specimens in which the pathogens were identified to be involved were respiratory specimens (n=189, 89.5%); bacteremia was detected in 22 cases (10.4%). The most common pathogens were Acinetobacter baumannii (n=68), followed by Pseudomonas aeruginosa (n=36), Klebsiella pneumonia (n=35), and Staphylococcus aureus (n=24). Moreover, MDR pathogens caused infection in 138 patients (70.4%), which had microbiologically diagnosed HAP/VAP. Furthermore, Acinetobacter species accounted for approximately half of the MDR pathogens, followed by Pseudomonas aeruginosa species (21.7%).

Bacterial pathogen identified in patients with hospital-acquired and ventilator-associated pneumonia
4. Treatment
An extended-spectrum penicillin/beta-lactamase inhibitor (59.3%) and respiratory fluoroquinolone (32.1%) are frequently used as initial empirical antibiotics (Table 4). Combination antibiotic therapy was provided to 249 patients (47.3%). Thereafter, adjunctive steroids were prescribed to 91 patients (17.3%). The median prednisone-equivalent dose was 50.0 mg (range, 25.0–75.0 mg), and the median treatment duration was 9.0 days (range, 3.0–22.5 days).
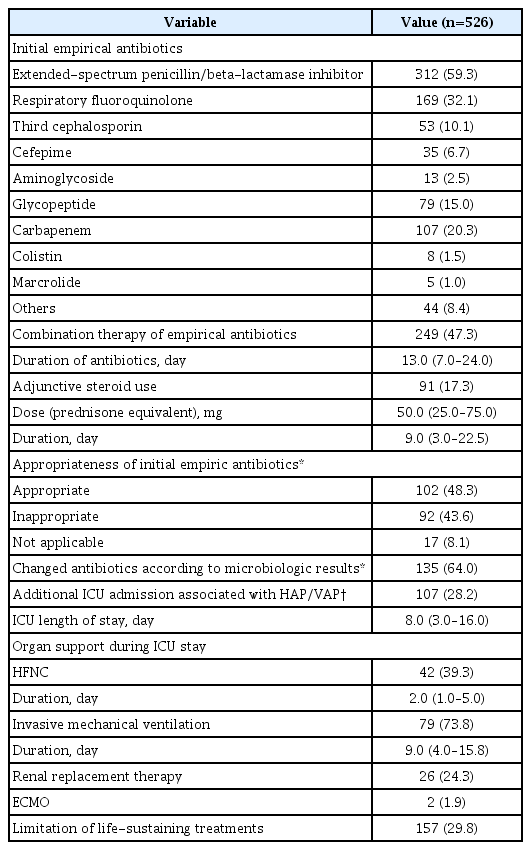
Treatment for hospital-acquired and ventilator-associated pneumonia
We diagnosed microbiological, clinical, and other possible infections in 211 (40.1%), 303 (57.6%), and 12 (2.3%) patients, respectively. Among the 211 patients with microbiological infections, an appropriate empirical antibiotic regimen was provided in 48.3% of the cases. Based on the susceptibility test, the antibiotics were changed in 135 patients (64.0%).
Among the 379 patients who were diagnosed with HAP in general wards, 107 patients (28.2%) were admitted to the ICU. The median length of stay in the ICU was 8.0 days (range, 3.0–16.0 days). During the ICU stay, 42 patients (39.3%) received high-flow nasal cannula therapy, while 79 patients (73.8%) received invasive MV. Extracorporeal membrane oxygenation was performed on two patients (1.9%).
5. Response to treatment and clinical outcomes
Among the total 526 patients, clinical cure, clinical failure, or the recurrence of pneumonia was observed in 344 (65.4%), 171 (32.5%), and 11 (2.1%) patients, respectively (Table 5). Furthermore, 183 patients were diagnosed with microbiological infections and were treated with follow-up cultures, but microbiological eradication was observed in only 106 (57.9%) patients.
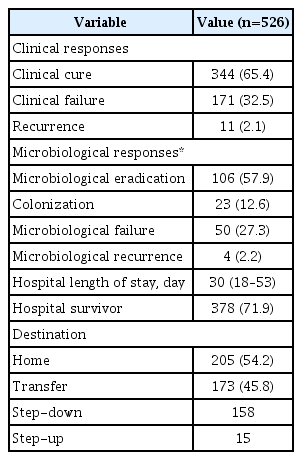
Clinical outcomes of patients with hospital-acquired and ventilator-associated pneumonia
The hospital mortality rate was 28.1%, and the median length of hospital stay was 30 days (range, 18–53 days). Among the patients who survived and were discharged from the hospital, 54.2% patients returned to their homes and 45.8% patients were transferred to other hospitals or similar facilities. Most of the referral cases were transferred to step-down care.
Discussion
In this study, we evaluated the clinical and microbiological characteristics, disease management, and the clinical outcomes of patients with HAP/VAP in Korea. The incidence of HAP/VAP was found to be 2.54/1,000 patients in Korea, and most patients (72.1%) were admitted to the general ward of the hospital. The pathogen involved was identified in 211 patients (40.1%), and MDR pathogens were detected in 70.4% of the included cases. An appropriate empirical antibiotic therapy was provided to 48.3% of the studied cases. Thus, clinical cure and microbiological eradication was observed in 65.4% and 57.9% of the studied cases, respectively. The hospital mortality rate was estimated to be 28.1%. Among the 378 patients who survived and were discharged, 54.2% were sent back home, while 45.8% were transferred to other hospitals or healthcare facilities.
In previous research studies on HAP/VAP, physicians focused on critically ill patients and patients who received MV. The results were used to develop and extensively implement evidence-based preventive care17. By implementing preventable care bundles, physicians could reduce the incidence of VAP and improve patient outcomes. Thus, the overall healthcare costs were reduced with this strategy18,19. In recent studies, physicians have diverted their attention to HAP patients that have been admitted to the general ward, that is, the non-ICU patients. Davis20 analyzed the data from the National Healthcare Safety Network, which is associated with the Centers for Disease Control and Prevention. The data was of patients diagnosed with complete nosocomial pneumonia. The retrospective study was conducted from January 1, 2013 through December 31, 2016. In this study, the total inpatient population was obtained from Pennsylvania acute-care facilities. Among these HAP patients, 60.9% cases were classified as non-ventilator HAP (NV-HAP) and 39.1% cases were classified as VAP. In this study, it was found that the mortality rates of VAP and NV-HAP cases were similar (22.5% vs. 20.3%) in 2016. Moreover, the total healthcare costs of VAP and NV-HAP cases was also similar in 2016 ($40,118,681 vs. $42,259,340). In addition, Giuliano et al.21 analyzed the 2012 United States National Inpatient Sample dataset and compared NV-HAP patients to patients with community-acquired pneumonia, non-pneumonia, or VAP cases. This study also proved that the total health care costs of NV-HAP cases was higher than that of other patients, with longer lengths of hospital stay and a greater likelihood of death as compared to all the groups, except for patients with VAP. In the present study, we also found that most of the HAP patients were diagnosed in general wards (72.1%). This indicates that most patients would be NV-HAPs in Korea. Therefore, physicians now emphasize on paying more attention to NV-HAP patients in general wards.
In this study, the most common pathogens were Acinetobacter baumannii (n=68) and MDR pathogens, which were documented in 70.4% of microbiologically confirmed HAP/VAP patients. The proportion of MDR pathogens involved in our study was higher than those included in recent HAP/VAP studies, which were conducted in other countries22–24. However, this increased proportion of MDR pathogens was in complete agreement with recent studies in Korea, including an epidemiological study of patients with sepsis25 and a single-center study of HAP in neurological patients26. As MDR pathogens are associated with an initial inadequate antibiotic treatment, the knowledge of local epidemiology is essential for assessing clinical outcomes27,28. Therefore, to develop domestic-specific guidance on HAP/VAP treatment, physicians must collect local microbiological data, including the prevalence of MDR pathogens.
For evaluating pathogens, positive blood culture is not usually used because it has a low sensitivity towards HAP/VAP29,30. Therefore, the guidelines for managing HAP/VAP recommend that respiratory specimens must be extracted with non-invasive or distal quantitative sampling2,3. In the present study, however, respiratory samples were not collected from all the patients. Conversely, blood culture tests were performed on a relatively large number of studied cases. Since the clinical judgment in the diagnosis of HAP/VAP is difficult31, careful efforts should be made to detect pneumonia in hospitalized patients with new or progressive parenchymal lung infiltrates in their chest radiograph. In contrast, when clinical findings suggest infection, physicians are compelled to extract respiratory specimens for adequate treatments, which are based on microbiological results.
In this study, the hospital mortality rate was 28.1%, which is lower than the mortality of studies with only VAP cases but higher than that of NV-HAP cases22,24,32. This finding may be related to the fact that the median age of patients with HAP/VAP was 71.0 years in this study. The severity of the disease is strongly associated with increased age and comorbidities that exist in aged patients33. In addition, as disability, frailty, and comorbidities are highly prevalent in elderly patients, leading to increased mortality rate34. In addition, among the patients who survived and were discharged from the hospital, 45.8% were transferred to hospitals or other facilities. This indicates that patients who suffered from HAP/VAP may encounter difficulties in returning to their daily lives, even after their survival. Therefore, frailty and comorbidities were highly prevalent in elderly patients, which might have compelled physicians to transfer them to other hospitals after acutely managing their HAP/VAP condition.
Although our study provided information about the prevalence, characteristics, and outcomes of HAP/VAP in Korea, there are several limitations that need to be mentioned. Firstly, given its observational nature, our findings remain prone to various biases. We used a national multicenter design to improve the generalizability of our findings, but there is a potential risk of selection bias. This is because we included only the patients who visited the tertiary or university-affiliated hospitals. Secondly, it is possible that we missed some of the HAP/VAP cases given that we used the International Classification of Diseases-10 code to screen the eligibility of study participants. Thirdly, this study was designed to evaluate the epidemiological features, and we did not collect the data pertaining to long-term outcomes. Future prospective studies of HAP/VAP should include a larger number of patients, and they must be followed up for a longer period of time. The results of these studies are needed to define the public health burden and economic impact of HAP.
In summary, the prevalence of HAP/VAP in adult hospitalized patients in Korea was 2.56/1,000 patients. In tertiary hospitals of Korea, patients with HAP/VAP were elderly and had a risk of aspiration. Therefore, they were often referred to step-down centers after the management of HAP/VAP. Additional epidemiological studies must be conducted and innovative health care policies must be designed to increase the awareness of HAP/VAP in citizens of Korea. With these measures, we can improve the clinical outcomes of those afflicted with HAP/VAP.
Notes
Authors’ Contributions
Conceptualization: Jeon K. Methodology: Ko RE, Min KH, Jeon K. Formal analysis: Ko RE, Min KH, Jeon K. Data curation: Hong SB, Baek AR, Lee HK, Cho WH, Kim C, Chang Y, Lee SS, Oh JY, Lee HB, Bae S, Monn JY, Yoo KH, Jeon K. Software: Ko RE, Min KH. Investigation: Ko RE, Min KH, Hong SB, Baek AR, Lee HK, Cho WH, Kim C, Chang Y, Lee SS, Oh JY, Lee HB, Bae S, Moon JY, Yoo KH, Jeon K. Writing-original draft preparation: Ko RE, Min KH, Jeon K. Writing-review and editing: Ko RE, Min KH, Hong SB, Baek AR, Lee HK, Cho WH, Kim C, Chang Y, Lee SS, Oh JY, Lee HB, Bae S, Moon JY, Yoo KH, Jeon K. Approval of final manuscript: all authors.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was funded by the 2019 Research Grant (2019-E2808-00), which was received from the Korean Disease Control and Prevention Agency.