The Influence of NAT2 Genotypes on Isoniazid Plasma Concentration of Pulmonary Tuberculosis Patients in Southern Thailand
Article information

Abstract
Background
Isoniazid (INH) is metabolized by polymorphic N-acetyltransferase 2 (NAT2) enzyme, which noticeably alters INH plasma concentration. We aimed to determine the distribution of NAT2 genotype in Thai tuberculosis (TB) patients and correlate their genotype with plasma INH concentrations.
Methods
Blood samples from 55 newly diagnosed pulmonary tuberculosis participants from three hospitals were collected to classify the subject by NAT2 genotype performed by the Multiplex haplotype-specific polymerase chain reaction method. Patients were grouped into three acetylators (fast, intermediate, and slow). On day 14 of tuberculosis treatment, the second blood sample was taken to estimate the peak plasma concentration at 2 hours after oral administration. INH plasma concentration was analyzed by liquid chromatography‒tandem mass spectrometry/mass spectrometry method.
Results
The NAT2 genotype distribution of fast, intermediate, and slow acetylator was 10.9%, 36.4%, and 52.7%, from six, 20, and 29 patients, respectively. The median (interquartile range) of INH plasma concentration at 2 hours post drug administration for these three genotypes were 0.75 (0.69–0.86), 2.56 (2.12–3.97), and 4.25 (3.56–5.50) µg/mL from four, 14, and 12 cases, respectively. The INH plasma concentration at 2 hours after administration was significantly associated with body weight and NAT2 acetylator.
Conclusion
The INH plasma concentration was found lower in fast than intermediate and slow acetylators. Body weight and NAT2 acetylator influenced INH plasma concentrations at 2 hours after drug administration. Therefore, the NAT2 genotype should be known before starting TB treatment to maximize therapeutic outcomes.
Introduction
The global treatment success rate for new tuberculosis (TB) decreased from 86% in 2013 to 83% in 2016 [1]. In Thailand, the treatment success rate was only 82% in 2016, while the country’s goal is 85% [1,2]. The first-line anti-tuberculosis drugs regimen for new TB patients containing isoniazid (INH), rifampicin (R), ethambutol (E), and pyrazinamide (Z) is a very high effective course of treatment [3]. Since the drug concentration varies noticeably among patients, the variation of drug concentration may lead to adverse drug reactions due to toxic drug levels on one extreme and the development of antibiotic resistance and treatment failure produced by suboptimal drug levels on another extreme [4].
INH, having a bactericidal effect on rapidly growing bacilli, is one of the most essential anti-TB drug for new TB patient [5,6]. N-acetyl transferase 2 (NAT2) is a deactivating enzyme for INH in the liver and small intestine. Its enzymatic activities are determined by the variation in single nucleotide polymorphisms of the coding region of exon 2 on NAT2 gene [7]. The human population is divided into three groups according to acetylation rate, i.e., fast, intermediate, and slow acetylators. Fast acetylators harbor NAT2*4 homozygous (wild-type) allele, intermediate acetylators carry the NAT2*4/*5B, *4/*6A, or *4/*7B dipotypes, and slow acetylators are lacking the NAT2*4 allele [8-10].
Low plasma concentrations of anti-TB drugs associate with human immunodeficiency virus (HIV) infection, age, sex, gastrointestinal tract disorders, body weight, diabetes mellitus (DM), and alcohol consumption [11-14]. Moreover, the host NAT2 enzyme activities affect the inter-individual variability in drug metabolism leading to low plasma concentrations of INH among fast acetylators [12]. Studies in several countries, including Thailand, found that the slow acetylation status based on genetic variants in the NAT2 gene markedly contributed to the mechanism of drug-induced hepatotoxicity [14-16].
The recent therapeutic drug monitoring (TDM) guideline for TB patients recommends measuring plasma concentration of INH collected at 2 hours after drug administration as the plasma INH level peaks around 2 hours after administration [4,11,17]. TDM is a beneficial approach to provide adequate drug doses and figure out drug-drug interactions, especially in TB patients who are slow responders to TB treatment or who have comorbidities [11].
The studies of INH plasma concentrations classified by NAT2 genotype among TB patients were published in some populations, it has been still limited in Thais. Therefore, in the present study, we aimed to determine the distribution of NAT2 genotype in new TB patients and correlate the genotypes with plasma INH concentrations. The study was conducted under routine conditions at TB clinic with a high number of TB cases in southern Thailand.
Materials and Methods
1. Study design
A prospective cohort study was conducted among patients with newly diagnosed pulmonary TB, aged between 18 and 65 years old, and receiving TB treatment. New TB outpatients were enrolled and gave informed consent at the TB clinic in Songklanagarind, Hat Yai, and Phatthalung hospitals from February 2018 to February 2019.
2. Eligibility criteria and study groups
TB patients were administered standard first-line anti-TB drug regimen based on their weight once daily. Recommendation dose of INH 4–6 mg/kg, rifampicin 8–10 mg/kg, ethambutol 15–20 mg/kg, and pyrazinamide 20–30 mg/kg. Moreover, vitamin B6, 50 mg daily, was given for the prevention of neuropathy from INH. Dosage formulation of all anti-TB drugs is a single separate tablet manufactured by the Government Pharmaceutical Organization (GPO), Thailand.
Exclusion criteria were as follows: (1) laboratory abnormality presenting before anti-TB drug treatment, (2) history of chronic hepatic illnesses such as cirrhosis, chronic hepatitis and viral hepatitis B or C, (3) pregnancy or lactation, (4) current alcohol drinker (within 1 month), (5) HIV positive, (6) prolonged use of steroid, (7) severe systemic debilitation, and (8) severe drug-interactions which affected INH plasma concentration. We further excluded patients after the initiation of anti-TB treatment who were resistant to INH, infected with non-tuberculous mycobacteria, and fail to continue anti-TB drugs.
3. Data collection
A questionnaire was used to collect demographic and clinical characteristics data. Blood tests for anti-HIV, liver function tests (albumin, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, total bilirubin, and direct bilirubin), viral hepatitis B and C were performed at the screening phase after consenting. A whole blood sample was drawn and kept in a 5-mL EDTA tube for NAT2 genotyping at the Department of Medical Science (DMSc). Acid-fast bacilli staining test, standard sputum culture, drug sensitivity test, and chest radiography were done before TB treatment.
4. Measurement of INH concentration
Fourteen days after anti-TB drug initiation, drug sampling was performed as the expected steady-state of anti-TB drug concentrations was reached. On the sampling day, two venous blood samples were collected from patients after fasting at least 8 hours before 2 hours after drug administration at the TB clinic. A blood sample of 3–5 mL was kept in a sodium heparin tube. Plasma was separated by centrifugation at 4°C and then stored at –80°C. It was transferred on dry ice to analysis at the laboratory in DMSc. Another sample was sent for the liver function tests. Any adverse drug reactions and drug compliance were interviewed.
5. NAT2 diplotyping method
NAT2 genotyping was determined by haplotype-specific polymerase chain reaction-based method [18]. Briefly, after DNA extraction from a whole blood sample using a commercial kit (QIAamp DNA blood mini kit, QIAGEN GmbH, Hilden, Germany), polymerase chain reaction (PCR) amplification was done in a total volume of 10 µL by using Bio-RaD T100 Thermal cycler (Hercules, CA, USA), initial denaturation at 95°C for 5 minutes, followed by 32 cycles of 95°C for 20 seconds, 64.5°C for 20 seconds, and 72°C for 30 seconds. Each DNA sample was amplified by six haplotype-specific primers (NAT2*4, *5B, *6A, *7B, *12A, and *13A) and internal control primers (TIMP1). NAT2 haplotypes were determined by direct visualizing of the specific size of PCR products in agarose gel after electrophoresis. The results NAT2 diplotypes (2 haplotypes) was then interpreted as acetylator (slow, intermediate, and fast) phenotypes. Fast acetylator phenotypes are homozygotes or heterozygous of high activity enzymatic haplotypes (NAT2*4, NAT2*12A, and NAT2*13A), while slow acetylators are those homozygote/heterozygous of low enzymatic haplotypes (NAT2*5B, NAT2*6A, and NAT2*7B). Heterozygotes of high and low enzymatic activity haplotypes were determined as intermediate acetylators.
6. Analysis of INH plasma concentration
INH plasma concentration was measured by high performance liquid chromatography‒tandem mass spectrometry using an ACQUITY UPLC H-Class system (Waters, Watford, UK) with a Kinetex XB-C18 column (2.1×100 mm, Phenomenex, Torrance, CA, USA). The flow rate was 200 µL/min. The mobile phases was isocratic of a mixture of 5 mM ammonium acetate in water (solvent A) and acetonitrile (solvent B). After protein precipitation with 50% Acetonitrile, the plasma samples were mixed with an internal standard (carbamazepine) and centrifuged at 4°C for 10 minutes. Total running time of 7 minutes with injection volume 1 µL for each sample. Drug concentrations were determined using a Xevo TQD (Waters). Quantification was achieved by multiple reaction monitoring in positive ion mode with transitions of m/z 138.20 to 121.10 and m/z 237.03 to 194.03 for INH and the internal standard, respectively. The linear assay range is 2–50 ng/mL (r2=0.99). Intra- and inter-day coefficients of variation are monitored to be lower than 10%.
7. Statistical analysis
Continuous variables were presented by median (interquartile range) for non-normal distributed data and mean±standard deviation for normally distributed data. The comparison of outcomes was made using Fisher exact test, Student’s t test, Wilcoxon rank-sum test according to the type of the variable with statistical significance defined at p<0.05. For multiple group comparisons, the analysis of variance (ANOVA) and Kruskal-Wallis test were used as appropriate. Univariate and generalized additive regression models (GAM) were performed to identify the factors associated with INH concentrations. All the analyses were performed using R software version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
8. Ethics consideration
This study was approved by the Research Ethics Committee of the Faculty of Medicine, Prince of Songkla University, Thailand (REC No. 60-378-18-1) before data collection. The directors of the involved hospitals gave their permission to conduct the research in each study setting. Participants provided written consent after an oral explanation concerning the study objectives and procedures.
Results
A total of 55 new patients with pulmonary TB were enrolled in the study. Twenty-five patients were excluded from further analysis because of INH resistance (n=5), hepatitis B virus surface antigen positive (n=1), failure to continue anti-TB drug treatment (n=1), loss to follow-up (n=1), failure to take medicines on time (n=7), and withdrawal (n=10). The total number of remaining patients for plasma drug concentration analysis was 30.
There were 10 of NAT2 genotypes among 55 new patients with pulmonary TB. The first three highest frequency of NAT2 genotypes were NAT2*4/*6A (25.5%), NAT2*6A/*6A (18.2%), and NAT2*6A/*7B (14.5%), respectively. Six patients (10.9%) having NAT2*4/*4 were classified as fast acetylator; 20 patients (36.4%) as intermediate acetylator with NAT2*4/*5B,*4/*6A,*4/*7B; and 29 patients (52.7%) as slow acetylators with NAT2*5B/*5B, *5B/*6A, etc. (Table 1).

Frequency and percentage of NAT2 genotype and acetylator in 55 new pulmonary TB patients
The blood samples from 30 patients were analyzed. Table 2 presents the demographics, clinical characteristics, and laboratory results of patients classified by NAT2 acetylator (fast, intermediate, and slow). The majority of TB patients were male. The mean age, body weight, body mass index among the three groups were not statistically different. Six of 30 (20%) had a history of contact TB patients in their families. All liver function test parameters and anti-TB drug doses were within the normal range at the onset of treatment.
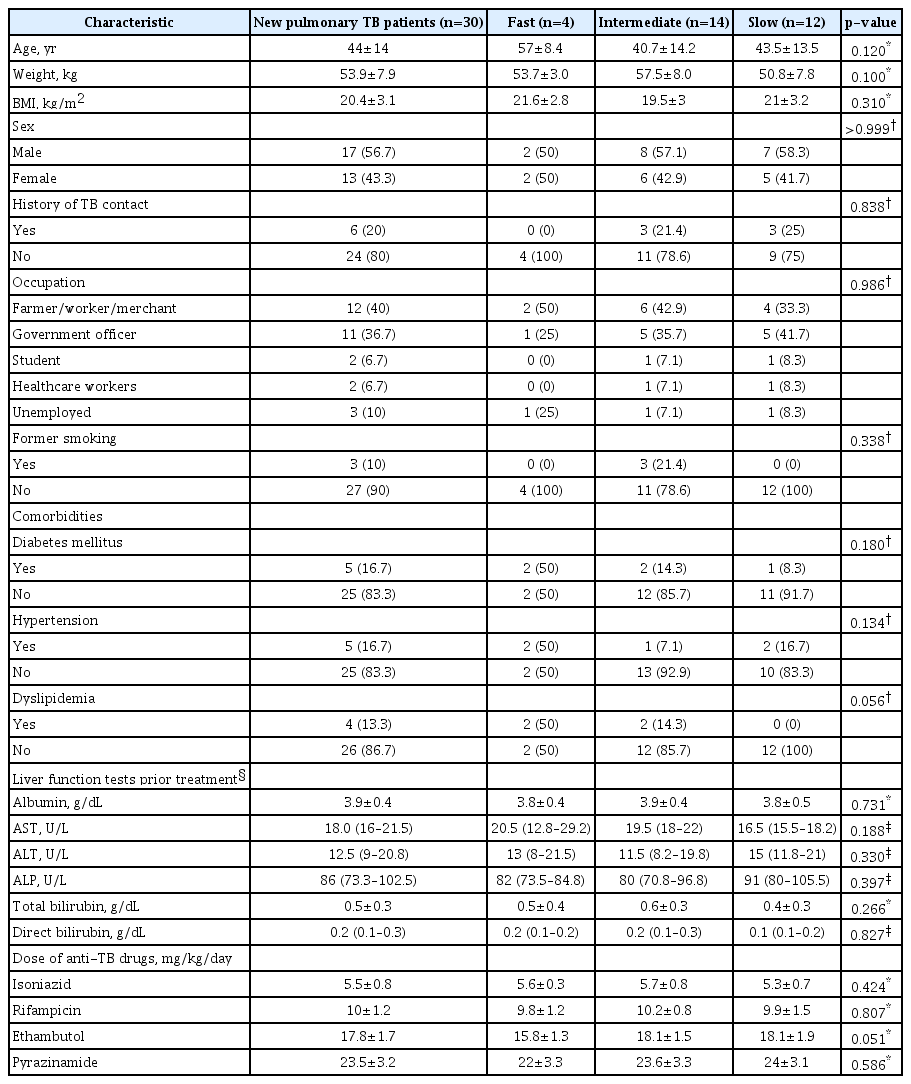
Patients’ demographics, clinical and laboratory information classified by NAT2 acetylator (fast, intermediate, and slow acetylator)
The frequency distribution of NAT2 phenotype group among tuberculosis patients with INH level as fast, intermediate, and slow acetylators was 4, 14, and 12 cases, respectively. Table 3 describes the median of INH plasma concentration at 2 hours after drug administration of 30 patients. NAT2*4/*4 genotype revealed the lowest INH plasma concentration at 2 hours after drug administration, while NAT2*6A/*6A genotype showed the highest INH plasma concentration at 2 hours after drug administration. The increase in median INH plasma concentration at 2 hours after drug administration across the three acetylator activities (fast, intermediate, and slow) is observed (Figure 1).

INH plasma concentrations at 2 hours after administration stratified by NAT2 genotype and acetylator

Comparison of isoniazid (INH) plasma concentration at 2 hours after administration among fast, intermediate, and slow acetylators. NAT2: N-acetyltransferase 2.
Age, sex, and height were not significantly associated with INH plasma concentration at 2 hours after drug administration by univariate analyses using ANOVA, t test, and linear regression, respectively. Dyslipidemia and NAT2 acetylator were associated with the INH plasma concentration at 2 hours after drug administration with a p-value of less than 0.05 in univariate analysis. The results from generalized linear model showed that the INH plasma concentration at 2 hours after administration was significantly in association with NAT2 acetylator and body weight, as shown in Table 4. The status of dyslipidemia was found highly associated with DM.

Results from generalized linear model between INH plasma concentration at 2 hours after administration and their covariates
Discussion
In this study, slow, intermediate, and fast acetylators were 52.7%, 36.4%, and 10.9% among new pulmonary TB patients. The results are similar to a study conducted mainly in the northern and central regions, which presented the percentage of slow, intermediate, and fast acetylators among non-hepatotoxic controls being 22.4%, 62.4%, and 15.3%, respectively [17]. While the percentage of fast acetylator is similar to our study, the proportion of the other two acetylators are different. However, another study in the northeastern region of the country showed a high frequency of fast acetylator (63.8%) among healthy Thais [19] as shown in Table 5. The difference in acetylator phenotypes in the four regions in Thailand has to be confirmed.

The distribution of NAT2 acetylator from different regions of Thailand
NAT2 acetylator status had been studied in some countries. The distribution of fast acetylator is similar among Caucasians (5.4%), Indians (7%), and Polish (10%) to Thais in the present study, whereas Chinese, Koreans, and Japanese are more frequent in fast acetylator of 40%–42.8% [4,8,20,21]. The proportion of slow acetylator in our study is similar to Europeans (Caucasians), Indians, and Africans. While South-East Asians (Malays, Filipinos, and Cambodians) are in the medium range of slow acetylator, but East Asians (Chinese, Koreans, and Japanese) have a low prevalence of NAT2 slow acetylator [4,20].
Due to genetic polymorphisms of NAT2, the results of this study show a significant difference in the INH plasma concentrations at 2 hours after administration in TB patients categorized by fast, intermediate, and slow acetylators, which is similar to the results of previous studies from Poland and Japan [8,16]. While the studies in Chennai [20] and Mumbai [22] have higher INH plasma concentrations at 2 hours after administration in three phenotypes than our study. In addition, NAT2*4/*4 genotype presented the lowest INH plasma concentration, while NAT2*6A/*6A genotype had the highest plasma concentration of the drug. The multivariate analysis revealed an effect of TB patient weight on INH plasma concentration at 2-hour post-administration as also shown in a previous report [23]. So, we could take NAT2 acetylator and body weight into account in estimating the INH plasma concentration at 2 hours post drug administration of which the expected INH plasma concentration
Studies from Brazil, Japan, UK, and Thailand [13,17,24,25] revealed that anti-TB drug induced hepatotoxicity was associated with slow acetylator; however, a study in China found no such relationship [26]. In the second week after anti-TB drugs administration, we found hepatotoxicity occurring in 4 of 29 slow and in 0 of 6 fast and 0 of 20 intermediate acetylators without significant difference owing to small numbers of the patients in each acetylator type. There were neither death nor serious adverse events during the study period. In contrast, fast acetylator has been suggested to result in the relapse, incomplete TB treatment, and drug failure due to sub-optimum plasma concentrations of INH in the previous studies [27,28]. Consequently, it is suggested that adverse drug reactions and treatment outcomes should be closely monitored in both slow and fast acetylators.
We designed the study on the basis of real clinical settings in TB patient management and kept a high standard laboratory test and specimen transfer. Firstly, we enrolled new TB patients who never took anti-TB drugs before and performed standard sputum culture for Mycobacterium tuberculosis to confirm TB cases and tested for the INH plasma concentration. Secondly, we kept samples on dry ice during transportation. We used a data locker to ensure the stability of temperature not being higher than –20°C during specimen transfer and storing at –80°C until analysis. Lastly, we ensured good compliance with anti-TB drugs of TB patients by telephone reminders and pill counts. Since this study focuses on the usefulness of the application of NAT2 genotyping on TDM of INH based on the physician and patient’s convenience, it underestimated the true peak concentration of INH (Cmax). Further studies on Cmax and area under curve from 0 to 8 h to clearly distinguish drug accumulation among these three NAT2 acetylators are suggested. Even we cannot control pharmacokinetic condition in real patients, the results of a cohort study are demonstrating the benefit of the use in a clinic setting with high biological and behavioral variation among patients and clinical conditions which can be treated in the variance of the statistical models. This study still had a limitation on the number of patients enrolled. Further study should enroll enough participants.
The results of this study suggest that NAT2 acetylator and body weight have a prediction power on INH plasma concentrations. The lower plasma concentration was found in fast than the other two groups of NAT2 acetylator. Therefore, the NAT2 genotyping should be done before starting TB treatment to optimize INH plasma concentration and reduce adverse drug reactions from INH.
Notes
Authors’ Contributions
Conceptualization: Ungcharoen U, Sriplung H, Mahasirimongkol S, Chongsuvivatwong V. Methodology: Ungcharoen U, Sriplung H, Mahasirimongkol S, Mokmued P, Chongsuvivatwong V. Formal analysis: Ungcharoen U, Sriplung H. Data curation: Ungcharoen U, Chusri S. Software: Ungcharoen U, Chongsuvivatwong V. Validation: Wichukchinda N, Mahasirimongkol S. Investigation: Chusri S, Chongsuvivatwong V. Writing - original draft preparation: Ungcharoen U, Sriplung H. Writing - review and editing: Ungcharoen U, Sriplung H, Wichukchinda N, Wattanapokayakit S, Mokmued P. Approval of final manuscript: all authors.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Funding
The study was supported by Fogarty International Center, National Institutes of Health -- Grant number D43TW009522.
Acknowledgements
This study was a part of the Master Thesis of the first author to fulfill the requirement for the TB/MDR-TB research training program at Epidemiology Unit, Prince of Songkla University. The authors would like to thank all medical staff at Songklanagarind, Hat Yai, and Phatthalung hospitals for their facilities and to care for participants; staff at the Department of Medical Science for analyzing NAT2 genotype and drug concentration; Assoc. Prof. Dr. Threerakamol Pengsakul for instruments and specimen storage; Mr. Surichai Bilheem for his assistance in statistical analysis.