Recent Advances in the Diagnosis and Management of Pneumocystis Pneumonia
Article information

Abstract
In human immunodeficiency virus (HIV)-infected patients, Pneumocystis jirovecii pneumonia (PCP) is a wellk-nown opportunistic infection and its management has been established. However, PCP is an emerging threat to immunocompromised patients without HIV infection, such as those receiving novel immunosuppressive therapeutics for malignancy, organ transplantation, or connective tissue diseases. Clinical manifestations of PCP are quite different between patients with and without HIV infections. In patients without HIV infection, PCP rapidly progresses, is difficult to diagnose correctly, and causes severe respiratory failure with a poor prognosis. High-resolution computed tomography findings are different between PCP patients with HIV infection and those without. These differences in clinical and radiological features are due to severe or dysregulated inflammatory responses that are evoked by a relatively small number of Pneumocystis organisms in patients without HIV infection. In recent years, the usefulness of polymerase chain reaction and serum β-D-glucan assay for rapid and non-invasive diagnosis of PCP has been revealed. Although corticosteroid adjunctive to anti-Pneumocystis agents has been shown to be beneficial in some populations, the optimal dose and duration remain to be determined. Recent investigations revealed that Pneumocystis colonization is prevalent and that asymptomatic carriers are at risk for developing PCP and can serve as the reservoir for the spread of Pneumocystis by airborne transmission. These findings suggest the need for chemoprophylaxis in immunocompromised patients as well as infection control measures, although the indications remain controversial. Because a variety of novel immunosuppressive therapeutics have been emerging in medical practice, further innovations in the diagnosis and treatment of PCP are needed.
Introduction
Pneumocystis jirovecii pneumonia (PCP) is a potentially life-threatening fungal infection that is seen in immunocompromised individuals12. Prior to 1980s, PCP was recognized as a rare but fatal infection primarily among patients with acute leukemia and other hematological malignancies. In 1980s, the worldwide epidemic of human immunodeficiency virus (HIV) dramatically increased the prevalence of PCP as one of its most common complications. Although PCP once increased explosively among HIV-infected patients, progress in antiretroviral therapies and the use of routine prophylaxis against PCP led to reduced rates of PCP in the HIV-infected population in most industrialized countries. However, the national database of the United Kingdom demonstrated an increase in the number of admissions due to PCP in patients without HIV infection3. This could be associated with the recent introduction of biologics and other immunomodulating agents for the treatment of rheumatic diseases, inflammatory bowel diseases, and malignancies4.
PCP develops in patients with immunosuppression or immunomodulation due to the underlying disease or its treatment. The underlying diseases or conditions of PCP in non-HIV patients include hematological malignancies, solid tumor, organ or hematopoietic stem cell transplantation, and connective tissue diseases under immunosuppressive treatment5. Risk assessments for PCP in these population are somewhat complex and cannot be clearly determined by CD4+ lymphocyte counts as in patients with HIV infection6. The most common treatment-related risk factors include the use of corticosteroids and other agents that modulate host immune reactions (Table 1). Whereas the diagnosis and management strategy of PCP in HIV-infected patients has been established, there are many issues to be solved concerning the diagnosis, treatment, and prophylaxis of PCP in non-HIV patients. This article will review the current understanding of the clinical features, diagnosis, treatment, and prophylaxis as well as infection control of PCP.

Immunosuppressive agents associated with the development of Pneumocystis pneumonia
Clinical Features of Pneumocystis Pneumonia
Clinical features of PCP are quite different between HIV-infected patients and those without HIV infection57. PCP in non-HIV patients is characterized by an abrupt onset of respiratory insufficiency. In non-HIV patients, it takes about a week from the onset of fever and dry cough until the development of respiratory failure, whereas PCP in HIV-infected patients has a more gradual disease course that lasts for 2 weeks to 2 months. Respiratory insufficiency is usually more severe in non-HIV patients than in HIV-infected population. Pneumocystis is more difficult to detect in non-HIV patients because of the smaller numbers of organisms in the lungs. The outcomes of PCP are more favorable in HIV-infected patients than in those without HIV infection. The mortality rates of PCP range from 30% to 60% among non-HIV patients, while it is 10% to 20% among HIV-infected population7.
These differences in the clinical features of PCP are thought to be owing to the differences in the immune response of the host89. Limper et al.8 reported that HIV-infected patients with PCP had significantly greater numbers of organisms and fewer neutrophils in bronchoalveolar lavage (BAL) fluid and less severe oxygenation impairment compared to other immunocompromised patients with PCP, which suggested that the severity of PCP could be determined by the inflammatory response rather than by the load of the organisms8. It was also reported that, the levels of inflammatory mediators in BAL fluid were higher in PCP patients without HIV infection than in those with HIV infection and inversely correlated with the oxygenation index9. Clinical features of PCP in non-HIV population are associated with severe or dysregulated inflammatory response evoked by a relatively small number of Pneumocystis organisms.
Diagnosis
1. Clinical presentation
PCP classically presents with fever, cough, and dyspnea, which are not specific to PCP. Compared with PCP in HIV-infected patients, PCP in non-HIV population usually develops more rapidly and causes more severe oxygenation impairment. Physical examination is nonspecific, and the pulmonary auscultation is often normal, even in the presence of significant hypoxemia10.
2. Microbiological diagnosis
Because Pneumocystis cannot readily be cultured in the laboratory, the microscopic demonstration of the organisms in respiratory specimens has been the golden standard for the diagnosis of PCP210. Cysts can be stained with Grocott-Gomori methenamine-silver, which has good specificity, but its sensitivity is not satisfactory. Because the trophic forms predominate over the cyst forms, Giemsa and Diff-Quik staining of the trophic forms is supposed to have high sensitivity, but it is not steady depending upon the skill and experience of the observer.
In non-HIV patients, bronchoscopic procedures for the diagnosis of PCP are often difficult due to rapidly progressive respiratory insufficiency411. In addition, PCP patients without HIV infection have a lower burden of Pneumocystis than those with acquired immune deficiency syndrome (AIDS), which leads to difficulty in detecting the organisms by microscopic observation4. Polymerase chain reaction (PCR) has 94%–100% sensitivity and 79%–96% specificity for the diagnosis of microscopically positive PCP1213141516. Due to its high sensitivity, PCR is increasingly used for the microbiological diagnosis of PCP. Although BAL fluid is the optimal specimen for PCR analysis, induced sputum has been shown acceptable. Moreover, it has been shown that Pneumocystis DNA can be detected by PCR in oropharyngeal washes and nasopharyngeal aspirates411.
Loop-mediated isothermal amplification (LAMP) is an established nucleic acid amplification method offering rapid, accurate, and cost-effective diagnosis of infectious diseases. Nakashima et al.17 retrospectively evaluated 78 consecutive HIV-uninfected patients who underwent LAMP method for diagnosing PCP. LAMP showed higher sensitivity (95.4%) and positive predictive value (91.3%) than PCR, indicating that Pneumocystis LAMP method is a sensitive and costeffective method and is easy to administer in general hospitals.
3. Serological diagnosis
Because BAL is often difficult for patients with respiratory failure, serological diagnoses of PCP have been investigated. (1→3)-β-D-glucan (β-D-glucan) is derived from the cell wall of several fungi including Pneumocystis18. The β-D-glucan assay was originally developed in Japan for diagnosis of deep-seated mycosis and has been best studied for Candida and Aspergillus spp.18. Although it is not specific for Pneumocystis, measurement of serum β-D-glucan level has been used for the diagnosis of PCP19202122. There remain, however, a couple of issues to be solved19. First, several different methods of measurement are commercially available, and they are not always compatible with each other. Second, false-positive results due to a number of factors, such as the administration of immunoglobulin, bacteremia, hemodialysis, surgical gauze exposure, and certain antibiotics, are known. Third, the cut-off value for the diagnosis of PCP still remains to be determined. In a retrospective case-control study of 295 patients with suspected PCP who had microscopy of BAL fluid for PCP and serum β-D-glucan assay with β-D-glucan Test Wako, Tasaka et al.20 found a cut-off value of 31.1 pg/mL with a sensitivity of 92% and a specificity of 86% for detecting PCP. On the other hand, Watanabe et al.21 evaluated the diagnostic value of the assay in 111 patients with AIDS and described a cut-off value of 23.2 pg/mL with a sensitivity of 96.4% and a specificity of 87.8%. de Boer et al.22 assessed the diagnostic accuracy in 31 non-HIV patients immunocompromised patients who were suspected of having PCP based on the clinical presentation and chest imaging. They showed that β-D-glucan measured by Fungitell was a reliable indicator for PCP with a sensitivity of 0.90 and specificity of 0.89 at the 60 pg/mL cut-off level22. Based upon these results, the β-D-glucan assay could be useful for the screening of the disease. In addition, serum β-D-glucan levels in patients with PCP were significantly greater than those in patients with colonization who had positive PCR results but improved without anti-PCP treatment, suggesting that the β-D-glucan assay may be helpful when considering treatment indication23. It remains controversial whether or how serum β-D-glucan assay is utilized for the assessment of treatment response or the prediction of the outcome of PCP2425.
Although elevated levels of serum lactate dehydrogenase and KL-6 and lower levels of plasma S-adenosylmethionine were noted in patients with PCP, the diagnostic significance of these markers has been shown to be inferior to that of β-D-glucan202226. Because this field has been intensely investigated, a standard for the serological diagnosis of PCP will be established in future.
4. Radiological presentation
On chest radiograph, PCP typically presents with bilateral or diffuse ground-glass opacity (GGO). Chest radiograph is sometimes normal. High-resolution computed tomography (HRCT) typically shows diffuse GGO with patchy distribution. In some patients with PCP, GGO is distributed in the subpleural lung parenchyma, whereas peripheral sparing of GGO occurs in others2728.
Differences in the radiological characteristics of PCP in patients with various underlying disorders had not been intensely investigated until Tokuda et al.29 reported the radiological features of PCP in patients with rheumatoid arthritis (RA) and PCP in HIV-infected patients. In a half of the RA patients with PCP, HRCT revealed diffuse GGO distributed in a panlobular manner, that is, GGO was sharply demarcated from the adjacent normal lung by interlobular septa (Figure 1A). The other half of the RA patients with PCP presented diffuse GGO without sharp demarcation, which is characteristic of PCP in HIV-infected patients (Figure 1B)29. In contrast, diffuse GGO distributed in a panlobular manner was rarely observed in PCP patients who received a biological agent for RA30. This difference in the HRCT patterns may result from difference in the host immune response.
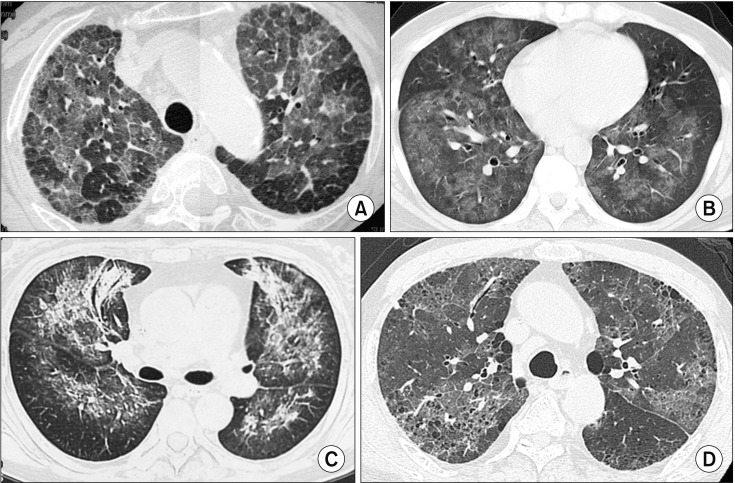
High-resolution computed tomography findings of Pneumocystis jirovecii pneumonia (PCP). (A) PCP in a patient with rheumatoid arthritis receiving methotrexate therapy. Diffuse ground-glass opacity (GGO) is distributed in a panlobular manner, in which GGO is sharply demarcated from the adjacent lung by interlobular septa. (B) PCP in a patient with human immunodeficiency virus infection. Diffuse GGO is distributed in an inhomogeneous manner without sharp demarcation. Subpleural sparing is also indicated. (C) PCP in a patient with malignant lymphoma. Among GGO, patchy consolidation is located along the bronchovascular bundle. (D) PCP in a cancer patient who was receiving chemotherapy and high-dose corticosteroid. Cysts are observed within the affected area, suggesting that they were formed by PCP.
PCP in patients with hematological malignancies is characterized by GGO with patchy consolidation along the bronchovascular bundle on HRCT (Figure 1C)31. Although cystic lesions were observed in similar percentages for both patients with HIV infection and those with malignancies (Figure 1D)31, other investigators described that cyst formation is a characteristic computed tomography finding of PCP in AIDS patients32. This discrepancy might be due to the fact that only limited data is available for the CT findings of PCP in patients with malignancies.
Treatment
Because of the high efficacy and the availability of oral and parenteral forms, trimethoprim (TMP)-sulfamethoxazole (SMX) is the first-line agent for the treatment of mild to severe PCP in both HIV-infected and non-HIV patients2101133. This therapy, however, is often complicated with adverse events, which include hepatotoxicity, nephrotoxicity, bone marrow depression, and skin rash, which sometimes becomes an obstacle to the completion of the treatment. The recommended daily dose is trimethoprim 15–20 mg/kg plus sulfamethoxazole 75–100 mg/kg33. Since this dose recommendation is not based on a randomized controlled trial, the optimal dose of TMP-SMX remains unclear. A retrospective investigation by Thomas et al.34 revealed a good outcome with trimethoprim 10 mg/kg/day plus sulfamethoxazole 50 mg/kg/day for PCP in HIV-infected patients. Kameda et al.30 reported that 67% of the rheumatic patients treated with TMP-SMX experienced adverse events, such as gastrointestinal and hematological disorders, and 38% could not complete the treatment. In their case series, the clinical outcome was favorable with only 4% of mortality, suggesting that a reduced dose of TMP-SMX may be sufficient for PCP in RA patients who were treated with a biological agent. In addition, Nakashima et al.35 retrospectively evaluated 24 consecutive patients without HIV infection who were diagnosed with PCP and treated with low-dose TMP-SMX (TMP 4–10 mg/kg/day; SMX 20–50 mg/kg/day). The low-dose group showed relatively high 30- and 180-day survival rates of 95.8% and 91.0%, respectively, with a high completion rate with the initial regimen (75.0%), indicating that low-dose TMP-SMX may be a treatment option for patients with non-HIV PCP.
Second-line agents include primaquine (30 mg/day) plus clindamycin (600 mg three times per day) or atovaquone alone (750 mg twice daily). Atovaquone is less effective but better tolerated than TMP-SMX36. Alternatively, intravenous pentamidine (4 mg/kg/day) can be given. Although pentamidine is about as effective as TMP-SMX, the incidence of adverse events, such as nephrotoxicity and dysglycemia, during treatment with pentamidine is even higher compared to TMP-SMX1137.
Putative TMP-SMX drug resistance is an emerging concern. Since this drug is widely used not only for treatment but also for prophylaxis, the emergence of drug resistance is anticipated. The inability to culture Pneumocystis in a standardized culture system prevents routine susceptibility testing and detection of drug resistance. In other microorganisms, sulfa drug resistance has resulted from specific point mutations in the dihydropteroate synthase (DHPS) gene. Similar mutations have been observed in P. jirovecii, and its association with prior sulfa prophylaxis failure has been reported38. Prevalence of these mutations has been increasing to as high as 81%39, although there has been no data showing significant association between the DHPS gene mutations and treatment failure211.
The recommended duration of treatment is 21 days in HIV-infected patients and 14 days in non-HIV immunocompromised hosts. Recommendation for longer treatment in HIV-infected patients is based on the higher organism burden and slower clinical response, which may result in a higher risk of relapse after only 14 days of treatment. In non-HIV patients, extended treatment should be considered in case of severe immunosuppression, high organism burden, or prolonged clinical improvement48.
In the guidelines, the addition of corticosteroids is recommended for HIV-infected patients with PCP33. Adjunctive corticosteroid therapy is advocated for PCP patients with arterial oxygen pressure less than 70 mm Hg because it could attenuate lung injury by blunting the inflammatory response initiated by the degradation and clearance of the organisms33. A systematic review showed a significant mortality-risk reduction with adjunctive corticosteroids in HIV-infected patients with PCP when substantial hypoxemia exists40. In non-HIV population, however, only a few retrospective studies have examined this matter414243. Pareja et al.41 found that non-HIV patients with severe PCP who received 60 mg or more of prednisone daily demonstrated favorable outcomes compared to those maintained on a low-dose corticosteroid regimen. They concluded that high-dose adjunctive corticosteroids might accelerate recovery in cases of severe PCP in adult non-HIV patients41. In another retrospective study, Korean investigators evaluated the outcomes of 88 non-HIV patients with moderate-to-severe PCP, comparing 59 patients with adjunctive corticosteroid use and 29 without42. As the survival analysis did not reveal any difference between the two groups, they concluded that adjunctive corticosteroid use might not improve the outcomes of moderate-to-severe PCP in non-HIV patients42. These diverse results may result from the heterogeneous background of the non-HIV subjects examined. Adjunctive corticosteroid use for PCP in a non-HIV patient should be considered after taking account of the background of the patient.
Prophylaxis
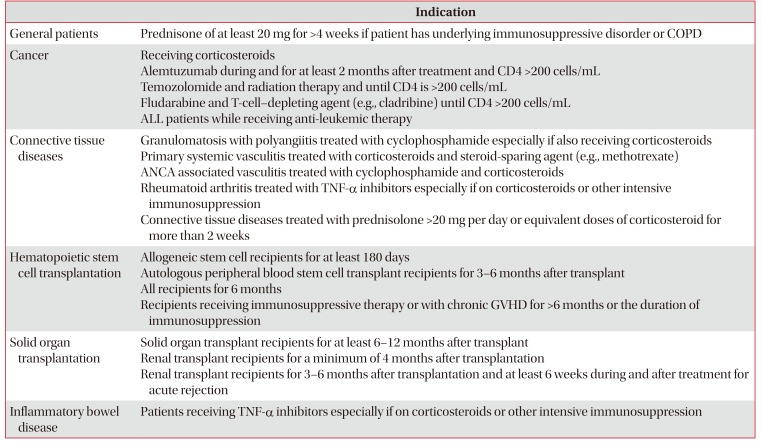
Despite intensive treatment, the mortality of PCP remains high, which is the rationale for chemoprophylaxis. There have been guidelines for the prophylaxis against PCP for patients with hematological diseases and solid tumors and recipients of hematopoietic stem cell transplantation and solid organ transplantation (Table 2)44454647. For immunocompromised patients with other underlying diseases, the indication and dosage for prophylaxis should be considered carefully, taking account of hepatotoxicity, bone marrow depress.

Proposed indications for chemoprophylaxis against Pneumocystis pneumonia
TMP-SMX is the first-choice prophylaxis in HIV-infected and in non-HIV immunocompromised hosts. The dosage usually recommended is one tablet (80 mg of TMP and 400 mg of SMX) daily or two tablets 3 times per week. Although the 3-times-weekly regimen was as effective in the prevention of PCP as the daily regimen, compliance may be enhanced by the daily regimen3648. In addition, Utsunomiya et al.49 recently reported a randomized controlled trial that evaluated the effectiveness and safety of a half-strength regimen (40 mg of TMP and 200 mg of SMX daily) in adult patients with systemic rheumatic diseases. No patients developed PCP by week 24, and the discontinuation rate was significantly lower in the half-strength regimen compared to the single-strength regimen (p=0.007), suggesting that the daily half-strength regimen might be optimal for prophylaxis of PCP in patients with systemic rheumatic diseases49. Alternative prophylaxis regimens include atovaquone (750 mg twice daily) or aerosolized pentamidine (300 mg once per month)36.
Two case-controlled studies showed that no PCP cases were identified in RA patients receiving salazosulfapyridine (SASP)5051. Although SASP has no antimicrobial effect, it may enhance Pneumocystis clearance by accelerating CD4+ T cell-dependent alveolar macrophage phagocytosis and by promoting TH-2 polarized cytokine environment leading to alternative macrophage activation52. The prophylactic effect of SASP remains to be confirmed by prospective studies.
Chemoprophylaxis is usually continued throughout the period of immunosuppression or as long as the risk lasts. Duration of the prophylaxis should be decided in a patient-based manner. In patients with RA or renal transplant recipients, a shorter period of prophylaxis may be sufficient4853.
Infection Control
P. jirovecii is a contagious airborne pathogen that can be transmitted among humans. Its DNA can be detected in the air surrounding PCP patients and asymptomatic carriers, suggesting P. jirovecii exhalation from them54. PCP outbreaks have been described, most of which have been observed among kidney or other solid organ transplant recipients55. Potential individual risk factors for PCP outbreak in renal transplant recipients were reported to be (1) frequent inpatient contact, (2) lack of adherence to isolation precautions, (3) the first year post-transplantation without chemoprophylaxis, (4) cytomegalovirus infection, and (5) age56. Therefore, preventing contact between such susceptible hosts and possible sources should be considered, especially in case of no chemical prophylaxis conducted. According to Centers for Disease Control and Prevention guidelines, a single-person wardroom for a PCP patient is preferred as well as the patient performing cough etiquette and wearing a mask when leaving the wardroom.
Prognosis
Mortality in non-HIV patients with PCP is 30% to 60%, whereas mortality rate ranges from 10% to 20% during the initial episode of PCP in HIV-infected patients1025. In non-HIV patients, the mortality depends on the population at risk, with a greater risk of death among patients with cancer than among patients undergoing transplantation or those with connective tissue disease72557. In addition, multivariate analyses revealed that low serum albumin levels and mechanical ventilation were independent predictors of mortality, which indicates that poorer general and respiratory conditions at diagnosis are associated with poor outcome of the patient31.
Conclusion
There still remain a lot of clinical issues regarding PCP in non-HIV population. For example, it is controversial how to utilize PCR for the diagnosis, how to use serum β-D-glucan testing as a diagnostic aid, and how and when to use adjunctive corticosteroids. The optimal dose of TMP-SMX and the indication and duration of chemoprophylaxis also remain to be investigated. Further efforts by investigators are warranted for better management of the disease.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.
Funding: No funding to declare.