Real-World Outcomes of Amikacin Liposome Inhalation Suspension for Refractory Mycobacterium avium Complex Pulmonary Disease
Article information

The burden of nontuberculous mycobacteria pulmonary disease (NTM-PD) is increasing, and Mycobacterium avium complex (MAC) are the most common etiology of NTM-PD [1]. MAC-PD is conventionally treated with macrolide-based multidrug regimens, although injectable aminoglycosides are recommended for advanced disease or macrolide-resistant cases. However, only approximately 60% of patients with MAC-PD achieve treatment success with the guideline-based therapy, while a substantial proportion of patients have refractory disease [2,3]. Recently, amikacin liposome inhalation suspension (ALIS), an inhalational formulation of amikacin that is packaged into liposomes, was developed [4]. ALIS, which can be delivered into the lung via aerosol nebulization, increases amikacin uptake into alveolar macrophages and limits systemic toxicities [5-7]. Evidence from the Amikacin Liposome Inhalation Suspension for Treatment-Refractory Lung Disease Caused by Mycobacterium avium Complex (CONVERT) study indicates an increased culture conversion rate for refractory MAC-PD after ALIS treatment [6,8]. Current guidelines recommend the use of ALIS for MAC-PD patients who have failed culture conversion despite more than 6 months of conventional regimens [9]. In South Korea, because the use of ALIS is not covered by the national health insurance, the cost burden is high (approximately $16,000/4 weeks), and therefore ALIS use is limited. In our institution, ALIS is usually used for advanced MAC-PD, refractory disease, and when an appropriate antibiotic combination is not possible. In this study, we aimed to describe our experience of using ALIS for refractory MAC-PD patients in a real-world clinical setting.
We evaluated six patients with refractory MAC-PD who started ALIS after failed culture conversion despite at least 10 months of conventional antibiotics, between January 2021 and December 2021 at the Samsung Medical Center, South Korea. A 590 mg dose of ALIS (Arikayce, Insmed Inc., Bridgewater, NJ, USA) was inhaled once daily using the LAMIRA nebulizer system (PARI GmbH, Midlothian, VA, USA) according to the manufacturer’s instructions. Sputum acid-fast bacilli (AFB) smear and culture were performed 1, 3, and 6 months after treatment initiation and then at 2- to 3-month intervals. Negative culture conversion was defined as at least three consecutive negative sputum cultures. The time of conversion was defined as the date of the first negative culture. Drug susceptibility testing was performed by measuring minimal inhibitory concentrations (MICs) using the broth microdilution method. Clinical, radiological, and microbiological data were retrospectively collected. Follow-up data were last updated in July 2022. This study was approved by the Institutional Review Board at the Samsung Medical Center (IRB no. 2022-09-024), and informed consent was waived.
Supplementary Table S1 shows the characteristics of the six patients at the time of starting ALIS. Of them, five patients had persistent positive cultures, and one patient (no. 5) showed radiological deterioration despite one negative culture result. Half of the patients were aged ≥65 years and had low body mass index (<18.5 kg/m2). Four of five patients with the nodular bronchiectatic form of NTM-PD had cavities, and one patient had the fibrocavitary form. Half of the patients had macrolide-resistant isolates, and more than half had isolates with high MIC values of ethambutol (≥8 μ/mL, 5/6) or rifampicin (≥8 μ/mL, 4/6) [10]. No patients had amikacin-resistant isolates. Prior to starting ALIS, all patients received conventional antibiotics (range 10.3 to 55.8 months) (Supplementary Table S2). They received macrolide/ethambutol-based regimens including rifamycin (n=5), clofazimine (n=5), moxifloxacin (n=3), linezolid (n=3), and intravenous amikacin (n=4), or nonliposomal amikacin inhalation (n=1).
Treatment outcomes of the study patients after starting ALIS are shown in Table 1, and detailed data for companion drugs are shown in Supplementary Table S3. One patient (no. 5) received ALIS for less than 3 months because the patient had one negative culture result at the time of adding ALIS and the patient maintained culture negativity and achieved radiological improvement. Three patients (no. 3, 4, and 6) received ALIS for less than 12 months because two of them were radiologically stable or improved, and the third patient (no. 4) achieved negative culture conversion at 1.1 months after ALIS. Two patients (nos. 1 and 2) did not show radiological improvement or culture negativity despite more than 12 months of ALIS, and so ALIS was discontinued. Serial changes in AFB smear and culture data at approximately 3-month intervals during the study period are shown in Supplementary Table S4.
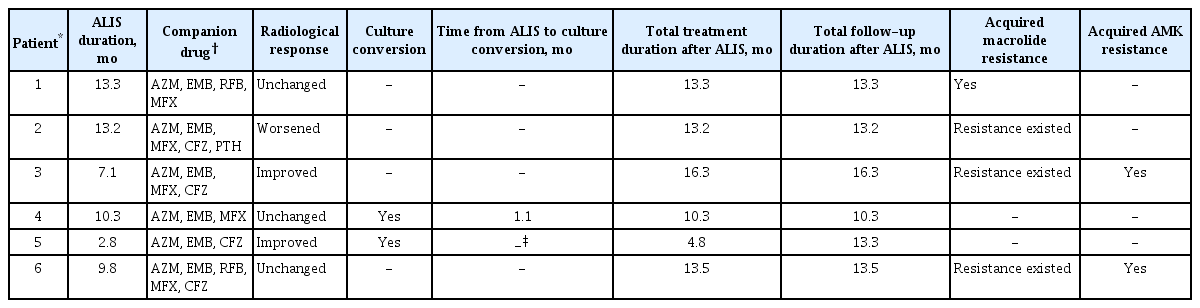
Treatment outcomes after starting ALIS in patients with refractory MAC-PD
In terms of outcomes associated with drug resistance, none of the patients with macrolide-resistant isolates (no. 2, 3, and 6) achieved culture conversion. Two of them developed amikacin-resistant isolates after the use of ALIS (no. 3 and 6), and among the MAC isolates, there was resistance to most of the companion drugs used, except clofazimine. One patient (no. 1) who had M. avium-PD that was macrolide susceptible, but resistant to both ethambutol and rifamycin, developed macrolide resistance after use of ALIS and failed to achieve culture conversion. Only one patient (no. 4) converted from positive to negative culture after starting the ALIS-containing regimen, and the patient had a macrolide- and amikacin-susceptible isolate and low bacterial burden (Supplementary Figure S1).
In our study, one patient experienced a cough after using ALIS, which was well controlled with an antitussive. In another patient, bloody sputum was observed at the beginning of ALIS use but spontaneously disappeared after 1 month.
In this study, we reported the treatment outcomes of ALIS-containing regimen for refractory MAC-PD in five patients with persistent positive cultures and one patient with radiological deterioration. Our data showed unsatisfactory outcomes in refractory MAC-PD even after adding ALIS. Only one patient (no. 4) achieved negative culture conversion, possibly because the patient had less advanced disease and macrolide susceptibility. Notably, in the patients who failed conversion, MAC showed high MICs to most of the companion drugs. Moreover, all three patients with macrolide-resistant MAC failed conversion, and two of them eventually developed amikacin resistance. The unsatisfactory outcome in our study (compared with the CONVERT study) could be explained by several factors, such as (1) real-world experience other than clinical trials, (2) the proportion of MAC isolates with clarithromycin resistance was 50% (it was approximately 20% in the CONVERT study) [8], and (3) five of six patients had a cavitary disease. Fortunately, in our study, there were no severe adverse effects, and ALIS showed long-term safety in the MAC-PD patients.
In conclusion, in this study, we investigated the additional effectiveness of ALIS in refractory MAC-PD patients. The addition of ALIS to standard treatment improved microbiological or radiological responses in some patients. However, for patients with macrolide-resistant isolates or cavitary lesions, the added benefit may be limited. Thus, further research on these findings is needed.
Notes
Authors’ Contributions
Conceptualization: Jhun BW. Methodology: Kim BG, Jhun BW. Formal analysis: all authors. Data curation: all authors. Software: all authors. Validation: all authors. Investigation: all authors. Writing - original draft preparation: Kim BG, Jhun BW. Writing - review and editing: all authors. Approval of final manuscript: all authors.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Funding
No funding to declare.
Supplementary Material
Supplementary material can be found in the journal homepage (http://www.e-trd.org).
Characteristics of study patients at the time of starting amikacin liposome inhalation suspension.
Antibiotics administered to study patients before starting amikacin liposome inhalation suspension.
Detailed data for companion drugs used with amikacin liposome inhalation suspension in patients with refractory Mycobacterium avium complex pulmonary disease.
Serial results of sputum AFB smear and culture with approximately 3-month intervals in study patients.
Chest computed tomography at the time of starting amikacin liposome inhalation suspension.