Successful Treatment of Tracheal Invasion Caused by Thyroid Cancer Using Endotracheal Tube Balloon Inflation under Flexible Bronchoscopic Guidance
Article information
Abstract
Tracheal invasion is an uncommon complication of thyroid cancer, but it can cause respiratory failure. A rigid bronchoscope may be used to help relieve airway obstruction, but general anesthesia is usually required. Tracheal balloon dilatation and stent insertion can be performed without general anesthesia, but complete airway obstruction during balloon inflation may be dangerous in some patients. Additionally, placement of the stent adjacent to the vocal cords can be technically challenging. An 86-year-old female patient with tracheal invasion resulting from thyroid cancer was admitted to our hospital because of worsening dyspnea. Due to the patient's refusal of general anesthesia and the interventional radiologist's difficulty in completing endotracheal stenting, we performed endotracheal tube balloon dilatation and argon plasma coagulation. We have successfully treated tracheal obstruction in the patient with thyroid cancer by using endotracheal tube balloon inflation and a flexible bronchoscope without general anesthesia or airway obstruction during balloon inflation.
Introduction
Because tracheal invasion caused by thyroid cancer usually involves the trachea adjacent to the vocal cords, intervention with a flexible bronchoscope is often difficult and even dangerous. Furthermore, the coughing resulting from the irritation of the severely narrowed airway can interfere with the procedure in the absence of general anesthesia. However, if a patient's condition is not stable enough to allow for general anesthesia, or if other palliative therapies are not available, a palliative procedure with a flexible bronchoscope under conscious sedation may be required to establish airway patency.
Recently, we treated tracheal invasion in a thyroid cancer patient by using endotracheal tube balloon inflation under flexible bronchoscopic guidance and conscious sedation. We report this case to share our experience, as our method is an alternative intervention that can be used to treat difficult tracheal obstructions.
Case Report
An 86-year-old female patient (145 cm, 35 kg) visited our hospital due to worsening dyspnea. Ten years prior, she was diagnosed with papillary thyroid cancer with invasion of the tracheal tissue, which was treated palliatively with a total thyroidectomy and radioactive iodine (RAI) therapy. Despite the RAI therapy, the thyroid cancer remained in the trachea, and the patient required further supportive treatment.
Six months prior, she was admitted to our hospital and underwent endotracheal intubation and mechanical ventilation due to respiratory failure. Computed tomography (CT) following intubation revealed an endotracheal mass filling the tracheal lumen. We recommended a palliative tracheostomy to wean the patient off the ventilator, but her family refused this procedure. Therefore, we decided to extubate and perform an endoscopic de-bulking procedure. During the bronchoscope-guided extubation, we found that the endotracheal mass was sufficiently compressed so as not to interfere with airway patency. Thus, we did not perform the bronchoscopic de-bulking intervention, and she was discharged with improvement.
To evaluate her current tracheal stenosis, a CT scan was performed. The results showed near-complete obstruction of the upper trachea by a cancerous invasion (Figure 1). We contacted the interventional radiologist to insert a tracheal stent under balloon dilatation, but he refused to perform the procedure due to the proximity of the mass to the vocal cords. We then recommended two procedures to the patient: a rigid bronchoscopy or a palliative tracheostomy under general anesthesia. The patient refused both recommended procedures, and a subsequent recommendation was made for an intervention employing a flexible bronchoscope. After the patient provided informed consent pertaining to the risks associated with a flexible bronchoscopic procedure, including respiratory arrest, electrical burn, and bleeding, intervention with the flexible bronchoscope was attempted to relieve her tracheal obstruction after injecting 3 mg of midazolam.

(A, B) Chest computed tomography (CT) at admission. Chest CT showing a endotracheal mass obstructing upper trachea (arrows).
The patient's upper trachea showed luminal narrowing of more than 75% of the diameter, 1.5 cm distal to the vocal cords, due to a polypoid mass with a soft consistency (Figure 2A). We attempted electrical snaring to reduce the cancerous mass in the trachea, but this procedure was not successful due to severe coughing. Next, we inserted an endotracheal tube with an 8.0-mm inner diameter through the narrowed lumen under bronchoscopic guidance. The cuff balloon, which was located in the narrowest part of the lumen, was maximally inflated for 15 seconds, after which the endotracheal tube was removed. Upon repeated flexible bronchoscopic examination, the endotracheal mass was found to be compressed (Figure 2B), and the patient's cough had decreased sufficiently to perform electrical snaring and argon plasma coagulation of the tumor. Immediately after the procedure, her dyspnea improved markedly (Figure 2C). Six hours after completion of treatment, flexible laryngoscopy was performed to evaluate the mobility of the vocal cords, and no immediate complications were noted. After 4 days of hospitalization, she was discharged. Tracheal patency has been maintained for 8 months.
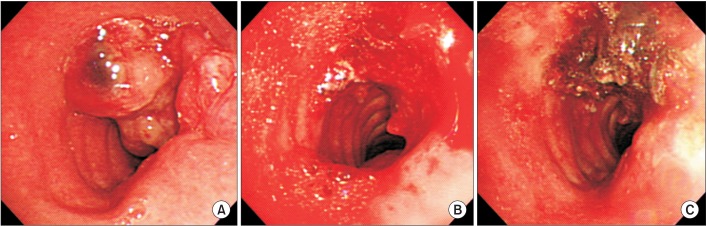
Bronchoscopic findings during procedure. Initial finding of upper trachea showing near total obstruction (A), tracheal luminal widening after endotracheal tube balloon inflation with bronchoscopic guidance (B), after argon plasma coagulation (C).
Discussion
Patients with inoperable thyroid cancers are usually treated by RAI therapy and external beam radiation therapy1. The role of oral RAI in airway invasion has not been investigated separately. Furthermore, a recent trial revealed that external radiation therapy had no clear benefits, and that routine external radiation therapy is therefore no longer recommended to treat inoperable thyroid cancer2. Chemotherapy is an alternative option in patients with inoperable thyroid cancer, but chemotherapy has limited efficacy for resolving airway obstructions.
In thyroid cancer with airway obstruction, a rigid bronchoscopic procedure with or without tracheal stenting is a good alternative method, but it is usually performed under general anesthesia. Thus, the equipment and facilities required for a rigid bronchoscopic procedure and general anesthesia are necessary3,4. The insertion of a tracheal stent by an interventional radiologist could also be used to relieve airway obstruction5,6, but it may be dangerous in patients with a mass abutting the vocal cords and may result in complications including stent migration, retained secretions, and stent fracture7.
Our patient had a tumor that did not respond to RAI, and she refused to undergo procedures under general anesthesia. Furthermore, we considered an endotracheal stent dangerous due to the very short distance between the mass and the vocal cords, so we were not able to perform endotracheal stenting under local anesthesia. During a previous flexible bronchoscopic intervention, the patient's mass was compressed with an endotracheal tube. We therefore decided to perform endotracheal intubation and balloon cuff inflation under bronchoscopic guidance. Previous studies reported successful endotracheal intubations in thyroid cancer with tracheal invasion8,9. Based on our experience and these reports, endotracheal balloon cuff inflation under bronchoscopic guidance may be a good alternative to treat tracheal obstruction resulting from thyroid cancer invasion.
We believe that endotracheal tube balloon dilatation has several advantages as a palliative procedure. First, there is no need for the equipment or facilities associated with rigid bronchoscopic procedures or general anesthesia. Second, maintaining adequate ventilation during endotracheal balloon dilation is easier, and a stepwise approach is also possible in some cases. Finally, it is believed that this method could greatly reduce the risk of complications that may arise when treating lesions of the upper trachea, closest to the vocal cords.
However, there are limitations to applying this procedure to all tracheal lesions. Endotracheal intubation may be difficult in severe airway obstruction with masses of a hard consistency, and the effect of balloon dilatation could also be limited in these cases. Additionally, because the treatment is performed under light sedation, patient movement and coughing are not completely suppressed. Thus, the precision of the procedure may be limited.
Our method could be applied to treat tracheal obstruction caused by an endotracheal tumor of a soft consistency, if the patient refuses to undergo surgery or bronchoscopic interventions under general anesthesia.
Notes
No potential conflict of interest relevant to this article was reported.