Development of Prediction Equation of Diffusing Capacity of Lung for Koreans
Article information
Abstract
Background
The diffusing capacity of the lung is influenced by multiple factors such as age, sex, height, weight, ethnicity and smoking status. Although a prediction equation for the diffusing capacity of Korea was proposed in the mid-1980s, this equation is not used currently. The aim of this study was to develop a new prediction equation for the diffusing capacity for Koreans.
Methods
Using the data of the Korean National Health and Nutrition Examination Survey, a total of 140 nonsmokers with normal chest X-rays were enrolled in this study.
Results
Using linear regression analysis, a new predicting equation for diffusing capacity was developed. For men, the following new equations were developed: carbon monoxide diffusing capacity (DLco)=−10.4433−0.1434×age (year)+0.2482×heights (cm); DLco/alveolar volume (VA)=6.01507−0.02374×age (year)−0.00233×heights (cm). For women the prediction equations were described as followed: DLco=−12.8895−0.0532×age (year)+0.2145×heights (cm) and DLco/VA=7.69516−0.02219×age (year)−0.01377×heights (cm). All equations were internally validated by k-fold cross validation method.
Conclusion
In this study, we developed new prediction equations for the diffusing capacity of the lungs of Koreans. A further study is needed to validate the new predicting equation for diffusing capacity.
Introduction
The advantages of physiologic tests for measuring diffusing capacity are that they permit diagnosis of an impaired surface area for transfer gases from the alveoli to the pulmonary capillaries, sometimes even during early stages of disease1. The diffusing capacity of the lung to exchange gas across the alveolar-capillary interface is determined by its structural and functional properties. A single breath carbon monoxide diffusing capacity (DLco) is commonly used to measure diffusing capacity of lung. So, the methodology of measuring diffusing capacity has been standardized in an attempt to ensure quality control and reduce between laboratory variability2.
In addition to the interlaboratory variability, the differences among prediction equations may also lead to misinterpretation of diffusing capacity3. Since the ethnic difference in diffusing capacity have been addressed in many studies4567, it is necessary to use the prediction equation of its own ethnicity.
In Korea, the prediction equation for diffusing capacity was developed in mid-80s8. However, this equation has not been widely used for interpreting the diffusing capacity even though this equation had been demonstrated to be clinically useful910. Instead, foreign prediction equations derived from Caucasians have been used1112131415.
The aim of this study was to develop a new prediction equation for diffusing capacity for Koreans using the data of Korean National Health and Nutrition Examination Survey1617.
Materials and Methods
1. Study design
This study was a part of quality control program of spirometry in 6th Korean National Health and Nutrition Examination Survey (KNHANES). The KNHANES is an ongoing surveillance system in the Republic of Korea that assesses the health and nutritional status of Koreans, monitors trends in health risk factors and the prevalence of major chronic diseases, and provides data for the development and evaluation of health policies and programs in Korea. The KNHANES uses rolling sampling survey method for the sample in each year to represent the whole nation and to be similar by years. Twenty households were selected throughout 192 regions each year and 10,000 individuals aged 1 year and over were targeted for KNHANES1617.
2. Study subjects
We recruited the life time non-smoker with normal spirometry results who were participating in KNHANES. The study subject also did not show any respiratory symptoms at least past 3 months and did not have any co-morbidities assessed by KNHANES. The study subjects also showed normal chest X-ray findings. The list of co-morbidities assessed by KNHANES were as followed: hypertension, hyperlipidemia, stroke, myocardial infarction, angina, osteoarthritis, rheumatic arthritis, osteoporosis, pulmonary tuberculosis, bronchial asthma, sinusitis, bronchiectasis, allergic rhinitis, depression, diabetes mellitus, and lung cancer.
We also excluded the subjects who had history of lung resection operation, congestive heart failure and other condition that might influence the result of diffusing capacity.
3. Procedures
1) Spirometry
Spirometry was performed using dry rolling seal spirometers (Model 2130; SensorMedics, Yorba Linda, CA, USA) and the American Thoracic Society (ATS)/European Respiratory Society (ERS) criteria for the standardization of pulmonary function test18. The results of spirometry in each enumeration districts were stored on web-hard to investigate whether the results satisfied acceptability and reproducibility criteria of spirometry for quality control and quality assurance. For analysis on results of spirometry, only results showing two or more acceptable curves and meeting reproducibility criteria were used17.
2) Measurement of diffusing capacity
After performing spirometry, eligible subjects, who were showing normal spiromety and chest X-ray result, were asked to participate in this study. When the subjects agreed to participate, informed consents were obtained. Then the subjects were transferred to regional teaching hospitals to perform diffusing capacity of lung test. A total of 16 hospitals participated in this study. The diffusing capacity tests were performed by experienced technicians who had at least 200 experiences of diffusing capacity test. Diffusing capacity was measured by single-breath technique using standardized method recommended by ATS/ERS recommendation using commercialized equipment (Autobox; SensorMedics)2.
The protocol of measuring diffusing capacity is briefly summarized as followed. The subject was seated comfortably throughout the test procedure. When the mouthpiece and nose clip were in place, tidal breathings were carried out for a sufficient time to assure that the subject is comfortable with the mouthpiece. After exhaling to the residual volume, the subject inspired the gas mixture rapidly to the total lung capacity (TLC), followed by breath-holding at full lung inflation and then performed rapid exhalation. A total of 85% of inspired volume was completed in <4.0 seconds. The breathhold time was 10±2 seconds, and the total exhalation time did not exceed 4 seconds (with sample collection time <3 seconds). We used only methane gas as tracer. The composition of inspired gas mixture was as followed: 0.3% CO, 0.3% CH4, 0.3% C2H2, 21% O2, balance N2. We adopted the acceptability and repeatability criteria proposed by ATS/ERS recommendation2. The average of two acceptable tests that meet this repeatability requirement was reported.
4. Analysis
Statistical analysis was carried out using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Data are presented as mean±standard deviation. We used regression equation to develop new prediction equation for diffusing capacity. Prediction equations for DLco and DLco/alveolar volume (VA) were derived separately for both sexes. The k-fold cross validation method was used to validate the regression equation. In cross validation, some of the data is used as a training set and the rest is used as a test set. A regression equation is made by using the training set and applied to the test set to validate the equation. Because the test set is not involved in the choice of the regression model, the performance of the regression equation in the test set can be a more accurate way to validate the usefulness of the regression model. In k-fold cross-validation, the original sample is randomly partitioned into k equal sized subsamples. Of the k subsamples, a single subsample is retained as the validation data for testing the model, and the remaining k-1 subsamples are used as training data. The cross-validation process is then repeated k times (the folds), with each of the k subsamples used exactly once as the validation data. The k results from the folds can then be averaged to produce a single estimation. The advantage of this method over repeated random sub-sampling is that all observations are used for both training and validation, and each observation is used for validation exactly once. Ten-fold cross-validation is commonly used. We also compared the predicted values of other reference equations81112131415.
5. Ethical statement
The study protocol was reviews and approved by the ethics and review board of each teaching hospital where the DLco was measured (Hallym University Sacred Heart Hospital, IRB No. 2015-I069). All study subjects provided written informed consent before taking DLco test.
Results
1. Demographic characteristics
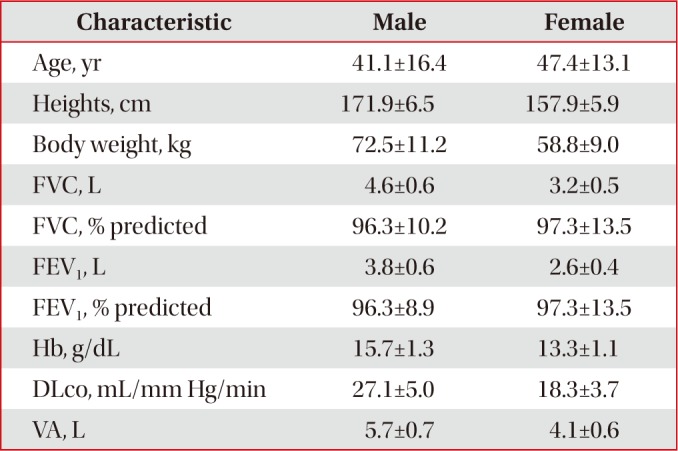
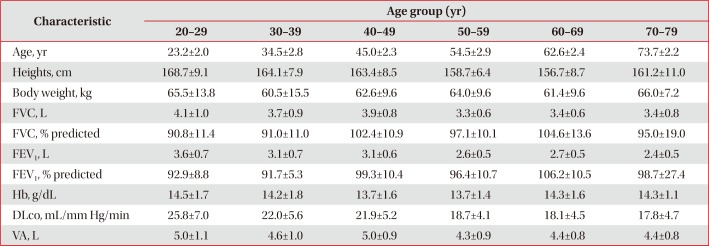
A total of 140 subjects (male 43, female 97) were enrolled in this study. The mean age of the study participants was 45.5±14.5 years. The age distribution of the study participants was as followed: 23 in 20s, 27 in 30s, 28 in 40s, 37 in 50s, 19 in 60s, and six in 70s. The mean values of forced vital capacity and forced expiratory volume in 1 second (FEV1) were 3.7±1.0 L and 3.0±0.7 L, respectively (Table 1). Tables 2 and 3 showed the baseline characteristics according to sex and age groups, respectively.

Baseline characteristics

Comparison of baseline characteristics according to sex

Comparison of baseline characteristics according to age groups
2. Development of new prediction equation for DLco
Bases on clinical significance and other prediction equations81112131415, we chose age, heights and body weight for the variables of the equation of DLco. The body weight was not sigificanct variable for the predication equation after multiple linear regression analysis (Table 4). Finally, we developed the new prediction equation for DLco and DLco/VA after adjusting hemoglobin (Hb) levels as below.

Development of new prediction equations for DLco and DLco/VA
For men,
For women,
The mean squared error obtained by k-fold cross validation test of DLco for men and women were 11.5 and 10.0, respectively.
3. Comparison of other prediction equations
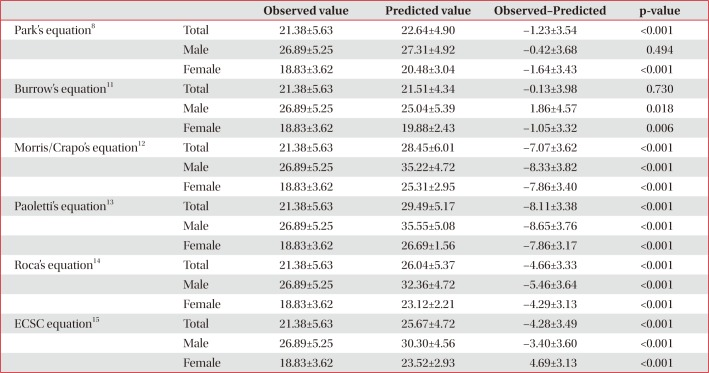
We calculated the difference of observed values and predicted values of other prediction equations. Except for Burrow's equations, all of other equations overestimated the diffusing capacity (Table 5).

The differences of predicted value and measured values of other equations
Discussion
In this study, we developed new prediction equations of DLco and DLco/VA using linear regression analysis after adjusting Hb levels following global standardized methodology2. For men, the following new equations were developed: DLco=−10.4433−0.1434×age (year)+0.2482×heights (cm); DLco/VA=6.01507−0.02374×age (year)−0.00233×heights (cm). For women, the prediction equations were described as followed: DLco=−12.8895−0.0532×age (year)+0.2145×heights (cm) and DLco/VA=7.69516−0.02219×age (year)−0.01377×heights (cm). Our new equations for DLco had positive association with heights and negative association with age in both sex. For the equation of DLco/VA, both age and heights had negative association. These associations were consistent with those from other prediction equations. Our new equation did not include body weight as a significant variable (Table 4), this finding was not new, because body weight excluded in many other prediction equations121315.
It is well known that Caucasians have higher lung volumes such as FEV1, vital capacity, and TLC compared to Asians5. Also, studies about the ethnic differences in DLco and DLco/VA showed that predicted values for the Chinese population were overestimated by the prediction equations from Caucasians46. We compared the predicted values from other prediction equations from Caucasians and the observed values. The differences of observed and predicted value were statistically significant in both sexes, which means that prediction equations from Caucasian ethnicity cannot be applicable for Koreans. We also calculated the predicted value from the old Korean prediction equation, and compared the observed values. The difference was also significant, especially in women (Table 5).
As this study enrolled subjects who were participating in the KNHANES, the study population could represent the whole Korean population. Therefore, there is no arguing about the representativeness of study population. So, the new prediction equations derived from this study can be applied in daily practice and used for constructing national database. The old Korean prediction equation was derived from single province of Korea with relatively short lists of exclusion criteria8 in spite of its usefulness910. Also, as the global standardization for measuring diffusing capacity has been addressed recently2, the old Korean equations could not follow the global standardization. However, a large study will be needed to validate the new prediction equations.
This study had some limitations. First is the relatively small number of participating subjects. Although the sampling strategy of present study was more strict than that of the study for prediction equation of spirometry19, the sample size was statistically adequate to generate the equations in both genders. And the second is the relatively young age of participating subjects. Lack of availability of sufficient number of normal elderly subjects who could perform acceptable test maneuvers was inevitable478. Therefore, caution is required in extrapolating these equations to elderly patients.
In summary, the prediction equations for DLco and DLco/VA were developed from the subjects participating in KNHANES. The age and heights were significant variables for the DLco. A further study is needed to validate the new predicting equation for diffusing capacity.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.