


Introduction
Chronic obstructive pulmonary disease (COPD) is a slowly progressive disease characterized as not fully reversible airflow limitation1. COPD occurs by various pathogenesis, and also has various clinical features. Thus, it is classified into various phenotypes2. The stage of COPD is classified according to forced expiratory volume in one second (FEV1). However, as this classification has a limitation in the prediction of the severity or prognosis of the disease, various evaluation indices such as the quality of life and body mass index (BMI), degree of airway obstruction and dyspnea and exercise capacity (BODE) has been used3-5. The acute exacerbation of COPD is considered an index that reflects the severity of the disease. However, it is still controversial for whether acute exacerbation of COPD is an important phenotype6. Accordingly, this study was conducted to investigate who are more susceptible to acute exacerbation and its correlation with disease severity. In addition, CD146, a marker of circulating endothelial cells that has been known to increase in patients with COPD in previous studies, was measured to investigate its correlation with acute exacerbation of COPD7,8.
Materials and Methods
1. Subjects
This study was conducted on COPD patients who visited the division of pulmonology of Gyeongsang National University Hospital from March 2010 to October 2010. Patients were diagnosed with COPD if FEV1/forced vital capacity (FVC) ratio was less than 70% after inhalation of short-acting bronchodilator according to the guideline on Global Initiative for Chronic Obstructive Lung Disease (GOLD). Subject inclusion criteria were as follows: current or ex-smokers with a smoking history of 10 pack years or higher, patients aged 40~80 years, and patients who were diagnosed with COPD and who had FEV1/FVC ratio<70%. Subject exclusion criteria were as follows: COPD patients with bronchial asthma, patients with structural pulmonary diseases such as severe bronchiectasis or tuberculous destroyed lung in chest X-ray, patients who were unable to complete a questionnaire themselves, patients who could not undergo 6-minute walk test, and patients with uncontrolled diseases that may affect study results. The subjects were divided into the frequent exacerbator group and infrequent exacerbator group, and then differences in clinical features were investigated between the two groups. Frequent exacerbator was defined as a patient with equal or more than two exacerbations per one year.
2. Methods
The subjects' age, gender, BMI, and smoking history were examined via the review of their medical records. As for the smoking history, the subjects were divided into the current smoker, ex-smoker, and never-smoker according to smoking status, and their total smoking amount was examined. The frequency of acute exacerbation for the recent one year was examined via the interview with the subjects. The Modified Medical Research Council (MMRC) scale was measured via a questionnaire. In this study, acute exacerbation was defined as an event requiring treatments with systemic steroid or antibiotics due to the rapid deterioration of respiratory symptoms such as cough, dyspnea, and sputum1. A pulmonary function test was conducted on all the subjects, and their disease stage was classified according to the GOLD guideline. 6-minute walk test was also conducted, and BODE index was measured. After achieving patients' informed consent, their blood samples were collected to measure CD146 level, a circulating endothelial cell marker. As for the measurement method, 10 mL of peripheral blood was collected from the subjects, and centrifuged to separate peripheral blood mononuclear cells. The peripheral blood mononuclear cells were then cultured with antibodies to CD146 for 30 minutes, followed by the quantitative analysis of CD146 using fluorescence activated cell sorting flow cytometry (Becton Dickinson and Company, Franklin Lakes, NJ, USA) and CellQuest software (Becton Dickinson and Company).
3. Statistical analysis
Each value was expressed as mean±standard deviation. An independent-samples t-test was conducted to compare pulmonary function, MMRC scale, 6-minute walk test, BMI, BODE index, and CD146 level between the frequent exacerbator group and infrequent exacerbator group. A chi-square test was conducted to compare gender, smoking history, and GOLD stage between the two groups.
The statistical analysis was conducted using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Differences were considered statistically significant if p<0.05.
Results
1. Basic characteristics of the subjects
A total of 60 COPD patients participated in the study. They consisted of 20 frequent exacerbators and 40 infrequent exacerbators. The subjects' mean age was 68.3±8.6 years and the male to female ratio was 57:3, which showed no significant difference between the two groups. The BMI was shown to be 21.3±2.4 and 22.6±3.9 in the two groups, respectively, which showed no significant difference. No significant difference in the previous and current smoking history was found between the two groups. In addition, no significant difference in the total amount of smoking was found between the two groups (45.3±38.9 pack years and 37.05±13.3 pack years, respectively) (Table 1).
2. Pulmonary function test
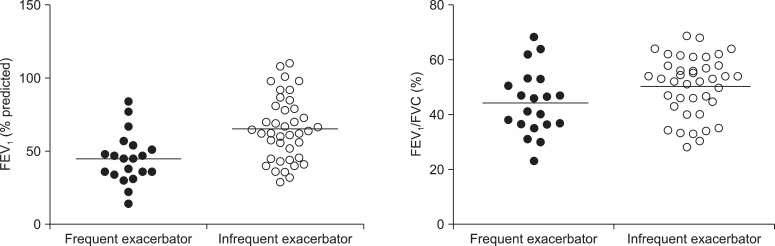
The COPD stage that was determined according to the GOLD guideline was shown to be significantly higher in the frequent exacerbator group (p=0.015) (Table 1). The mean FEV1 of the frequent exacerbator group was shown to be 45.0±17.2% and that of infrequent exacerbator group was 65.3±21.8% (p=0.001). The FEV1/FVC ratio was shown to be 44.3±11.9% and 50.5±10.8% in the two groups, respectively, which was significantly lower in the frequent exacerbator group (p=0.046) (Figure 1).
3. BODE index
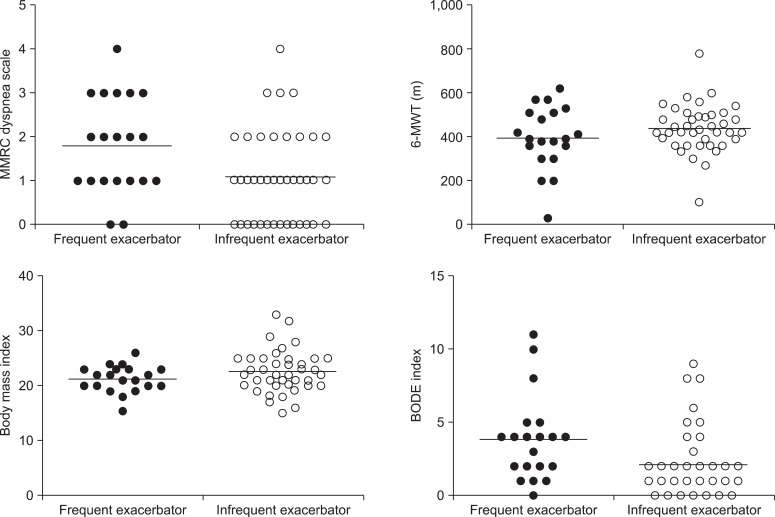
The MMRC scale was shown to be 1.8±1.1 and 1.1±1.0 in the two groups, respectively, which was significantly higher in the frequent exacerbator group (p=0.016) (Figure 2). 6-minute walk test and BMI showed no significant difference between the two groups (p=0.198 and p=0.162) (Figure 2). As a result of calculating the BODE index, it was shown to be 3.9±2.9 in the frequent exacerbator group, and 2.1±2.3 in the infrequent exacerbator group, which was significantly higher in the frequent exacerbator group (p=0.014) (Figure 2).
4. CD146
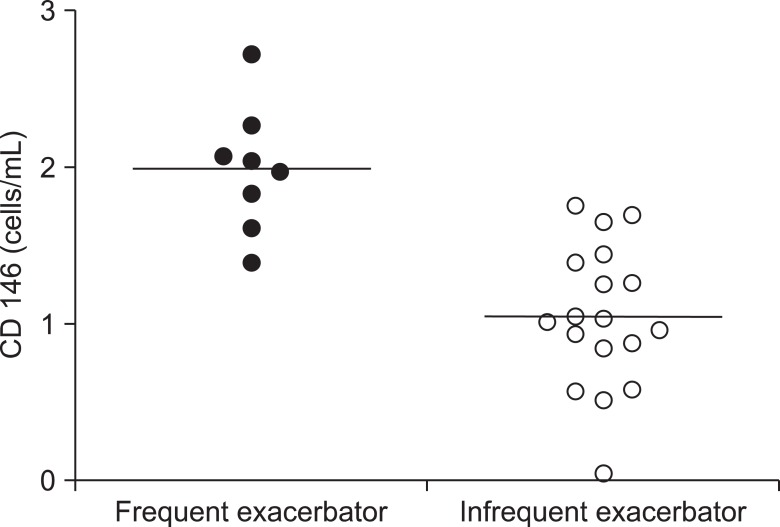
Twenty-six out of the 60 subjects agreed to blood collection, of whom eight subjects were frequent exacerbators and 18 subjects were infrequent exacerbators. The mean concentration of CD146 was shown to be 2.0±0.4 cells/mL in the frequent exacerbator group, and 1.0±0.5 cells/mL in the infrequent exacerbator group, which was significantly higher in the frequent exacerbator group (p<0.001) (Figure 3).
Discussion
In this study, the COPD patients were divided into the frequent exacerbator group and infrequent exacerbator group, and then differences in the clinical features and CD146, a circulating endothelial cell marker, were compared between the two groups. Despite the unclear establishment of the definition of the acute exacerbation of COPD, the definition described in the GOLD guideline has been most commonly used. Thus, in this study, the definition was used according to the GOLD guideline1. In addition, the classification of frequent exacerbator group and infrequent exacerbator group has not been clearly established. Thus, in this study, the subjects were classified according to the mean frequency of acute exacerbation for the past one year. As shown in a study conducted by Hurst et al.9, the subjects were classified into the frequent exacerbator group if they had acute exacerbation twice or more during the past one year. The results of this study showed that the airway obstruction was more sever in the frequent exacerbator group than in the infrequent exacerbator group, and that the BODE index and CD146 concentration were higher in the frequent exacerbator group than in the infrequent exacerbator group.
Miravitlless et al.10 reported that the risk of acute exacerbation increased as airway obstruction became more severe. Cote et al.11 reported that airway obstruction was more severe in the patients with acute exacerbation than in the patients without acute exacerbation, and also reported that airway obstruction was more severe in the patients who had acute exacerbation twice or more than in the patients who had acute exacerbation once in a prospective study that was conducted on 205 COPD patients for 24 months. In this study, the disease stage according to the GOLD guideline was higher in the frequent exacerbator group than in the infrequent exacerbator group. In addition, the FEV1 and FEV1/FVC were lower in the frequent exacerbator group, which were consistent with the results of previous studies.
BODE index is comprised of FEV1, BMI, 6-minute walk test, and MMRC scale4. Cote et al.11 reported that BODE index was higher in patients with acute exacerbation than in patients without acute exacerbation. Hodgev et al.12 reported that the frequency of acute exacerbation had a significant correlation with BODE index, and that the BODE index was higher in the frequent exacerbator group than in the infrequent exacerbator group. In this study, the BODE index was higher in the frequent exacerbator group than in the infrequent exacerbator group, which indicates that acute exacerbation may more frequently occur in patients with high BODE index. No significant difference in the BMI and 6-minute walk test that are components of BODE index was found between the two groups in this study. Donaldson and Wedzicha13 and Cote et al.11 also reported that no significant difference in BMI and 6-minute walk test was found between the infrequent exacerbator group and frequent exacerbator group. On the other hand, Cote et al.11 reported that MMRC scale was higher in patients who had acute exacerbation twice or more than in patients who had acute exacerbation once for 24 months. In this study, the MMRC scale was also shown to be significantly higher in the frequent exacerbator group than in the infrequent exacerbator group.
Smoking is a major causative factor of COPD by deteriorating pulmonary functions. Vestbo et al.14 reported that smoking additionally caused annual reduction of pulmonary function of 21±4 mL in a study conducted on patients with moderate to severe COPD. Au et al.15 reported that smoking cessation reduced the frequency of acute exacerbation in COPD patients, and that risk reduction was correlated with period of smoking cessation in a study conducted on current and ex-smokers. However, no significant difference in the current and previous smoking history and smoking amount was found between the two groups in this study.
Circulating endothelial cell is an index that represents endothelial damage and dysfunction. It has been known to increase in patients with cardiovascular diseases such as acute myocardial infarction, pulmonary arterial hypertension, and stroke16-19. In addition, it has been reported to increase in patients with Behcet's disease, vasculitis such as systemic lupus erythematosus, infectious diseases such as sepsis, and various type of tumors20-23. Circulating endothelial cells have been known to increase in patients with COPD7,24. Sala et al.8 reported that circulating endothelial cells more increased in patients with acute exacerbation than in the control and patients with stable chronic pulmonary disease. Meanwhile, no study on the relationship between frequency of acute exacerbation and circulating endothelial cells has been conducted yet. In this study, the CD146 concentration was shown to have more increased in the frequent exacerbator group than in the infrequent exacerbator group, which showed that systemic vascular injury and dysfunction were more severe in the frequent exacerbator group.
In conclusion, compared to the infrequent exacerbator group, the frequent exacerbator group had more severe airway obstruction, higher BODE index, and higher CD146 level. Based on the aforementioned results, the acute exacerbation is likely to be one of the important phenotypes of COPD and a further study on CD146 is required.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






