


Introduction
Smoking causes cancer, cardiovascular diseases, and pulmonary diseases. It is the most important causative factor of the aforementioned diseases and can be prevented. In advanced countries, smoking has been known to account for 35% of the total death caused by cancers and for 90% of death caused by lung cancer1. In particular, the risk of lung cancer has been known to increase in proportion to the duration and amount of smoking2. According to 2008 Korea National Health and Nutrition Survey, the smoking rate of Koreans was reported to be 47.7%, 7.4%, and 27.7% for men, women, and both men and women, respectively, which is relatively higher than that of US (smoking rate of adult males 19%, smoking rate of adult females 15%, total smoking rate 17%) or France (smoking rate of adult males 28%, smoking rate of adult females 19%, total smoking rate 23%)3. The reason for high smoking rate despite the well-known harmfulness of smoking is attributable to addiction caused by nicotine contained in cigarette. Nicotine acts on the compensation circuit of the brain, causing addiction and resistance by physical and psychological dependence. Thus, it is difficult to initiate and maintain smoking cessation for oneself4,5. Thus, it is necessary to perceive smoking as a disease which should be managed and treated such as drug addiction or chronic diseases rather than as a personal habit or hobby, or to rely on personal decision or will to quit smoking.
Varenicline, which is a smoking cessation aid that has been developed for smoking cessation, is a partial agonist of ╬▒4╬▓2 nicotine receptor6. Varenicline stimulates nicotine receptors, making the receptors release a small amount of dopamine, thereby reducing smoking desire and withdrawal symptoms. In addition, as varenicline inhibits the binding of nicotine to nicotine receptors, dopamine releasing effect caused by nicotine is suppressed despite smoking, which results in no satisfaction by smoking7,8. Varenicline is recommended to be treated for minimum 12 weeks. A randomized study, which was conducted during 12-week non-treatment period after 12-week varenicline treatment, reported that the success rate of 6-month smoking cessation was 46.8%, which was significantly better than 21.8% observed in the placebo group9. However, smoking cessation aids such as varenicline are not covered by medical insurance in Korea. Thus, smokers are financially burdened, and the drug compliance of smokers is low as shown in a situation where smokers would rather quit smoking by themselves than believe the efficacy of drug even if smoking cessation aids are prescribed. Thus, in many cases, varenicline is not treated for 12 weeks. Accordingly, this study was conducted on smokers who received varenicline in the smoking cessation clinic of a general hospital health care center to analyze the characteristics of the subjects and to investigate the effect of varenicline treatment period on the success rate of 6-month smoking cessation.
Materials and Methods
This study was conducted on 87 subjects who received varenicline of 105 smokers who visited the smoking cessation clinic of Samsung Medical Center from September, 2007 to December, 2009. Among the 87 subjects, 9 subjects who failed follow-up 6 months after study initiation were excluded. At the first visit, the subjects were asked to complete a self-reported questionnaire for items such as educational background, income level, stress severity at home and in a working place (the Korean Psychological Well-being Index [SF-PWI; 18 items])10, presence of underlying diseases including psychiatric diseases, number of drinking, motives for smoking cessation, age of smoking commencement, smoking duration, mean daily smoking amount, reasons for smoking, previous history of smoking cessation and methods, reasons for the failure of smoking cessation, reasons for current smoking cessation trial, presence of smokers in the family, and nicotine dependence, followed by an interview with a specialist. The subjects were educated to know that smoking is a disease caused by nicotine addiction via multimedia to provide smoking cessation motivation. Exhaled CO concentration was measured using a device measuring exhaled CO concentration, and a consultation about determining anticipated smoking cessation date, writing smoking cessation diary, measures to withdrawal symptoms, and smoking cessation methods was conducted on the subjects. The subjects were asked to visit the clinic every 2 weeks for the first month after their enrollment to the smoking cessation clinic, and thereafter once a month to undergo measurements of physical factors and exhaled CO concentration, and medical and nutritional consultations. They were asked to receive varenicline at a dose of 0.5 mg from day 1 to day 3 once a day, and at a dose of 0.5 mg from day 4 to day 7 twice a day, and at a dose of 1 mg starting from the second week twice a day according to the recommendation of drug use. Non-smoker was defined as a subject who orally reported that he/she did not smoke at all and who showed that the result of measuring exhaled CO level was within the normal range. Smoking cessation success was defined as a subject who maintained smoking cessation for 6 months or longer. This study was conducted after approved by the clinical study center of Samsung Medical Center.
1. Statistical methods
A statistical analysis was conducted using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) and SAS (SAS Institute Inc., Cary, NC, USA). Median (quartiles) was used for the expression of statistics. A logistic regressional model was used for the analysis of factors affecting the success of 6-month smoking cessation and effects of varenicline treatment on the success of 6-month smoking cessation.
Results
1. Characteristics of the subjects
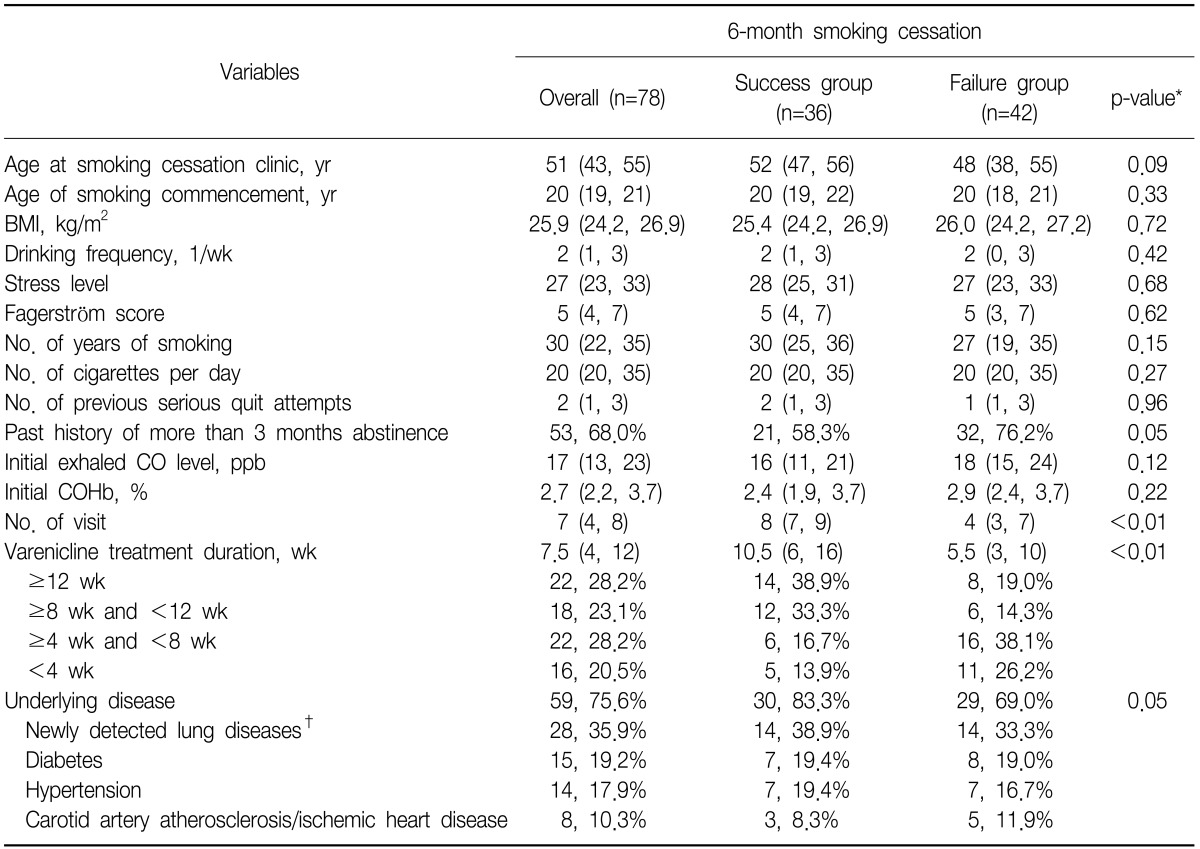
A total of 78 subjects were all males with a mean age of 48 years (range, 23~64 years) (Table 1). They consisted of 13 subjects with an age of 39 years or lower, 25 subjects with an age of 40~49 years, 33 subjects with an age of 50~59 years, and 7 subjects with an age of 60 years or higher. Subjects in their 40~50s accounted for 74%, which was the highest. The mean age of smoking commencement was 20 years. Sixty-four percent of the subjects commenced smoking before an age of 29 years, and smoked averagely 26 cigarettes a day, and had a smoking history of 28 years. Eighty-three point six percent of the subjects had educational background of university or higher and 85.2% of the subjects had a monthly income of 4 million won or higher. Varenicline was treated to 22 subjects (28.2%) for 12 weeks or longer, 18 subjects (23.1%) for 8~12 weeks, 22 subjects (28.2%) for 4~8 weeks, and 16 subjects for less than 4 weeks among the total 78 subjects.
2. Analysis of the success rate of 6-month smoking cessation and factors affecting the success rate of smoking cessation
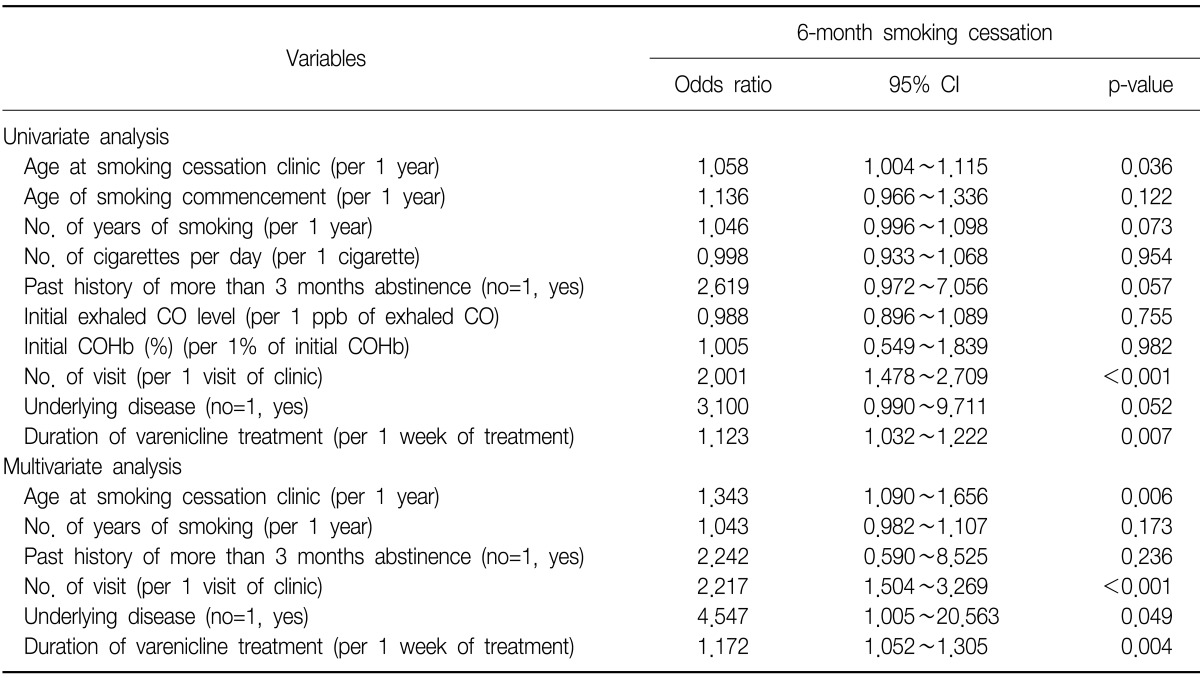
The success rate of 6-month smoking cessation of the 78 subjects was shown to be 47.4%. Based on the 12-week varenicline treatment, the success rate of 6-month smoking cessation was shown to be 63.6% in the group that received varenicline for 12 weeks or longer, which was higher than 41.1% of the group that early terminated varenicline treatment (less than 12 weeks) (p=0.074). As a result of univariate analysis, factors affecting the success rate of 6-month smoking cessation were shown to be age at the time of visiting the smoking cessation clinic, total number of visiting the smoking cessation clinic, presence of underlying diseases, and varenicline treatment duration (Table 2). A multivariate analysis showed that the odds ratio of 6-month smoking cessation success increased to approximately 1.34-folds and 2.22-folds in the cases of higher age at the visit of the smoking cessation clinic and an increase in the number of visiting the smoking cessation clinic, respectively, if other factors were constant. In addition, the odds ratio of 6-month smoking cessation success was approximately 4.55-folds higher in the case of underlying diseases compared to that of no underlying disease. However, when the underlying diseases were classified into pulmonary nodules, hypertension, diabetes, and carotid artery atherosclerosis/ischemic heart disease, and then analyzed again, no significant difference was found.
When the period of varenicline treatment was extended one more week, the odds ratio of 6-month smoking cessation success was shown to have increased to approximately 1.17-folds (p=0.004; 95% confidence interval [CI], 1.052~1.305). Compared to the group with varenicline treatment less than 4 weeks, when the varenicline treatment period was classified into less than 4 weeks, 4~8 weeks, and 8 weeks or higher, and analyzed, the odds ratio of 6-month smoking cessation success significantly increased to approximately 5.08-folds in the group with varenicline treatment for 8 weeks or higher (p=0.011; 95% CI, 1.362~18.925), but insignificantly increased to approximately 2.18-folds in the group with varenicline treatment for 4~8 weeks (p=0.477; 95% CI, 0.495~9.619).
3. Adverse events caused by varenicline
Twenty-eight cases of adverse events were observed in 24 subjects (30.8%) among 78 subjects who received varenicline. They included nausea (14.1%, 11/78), abnormal dreaming (5.1%), weakness (2.6%), headache (2.6%), insomnia (2.6%), unknown loss of consciousness, abnormal blood pressure elevation, abdominal pain, itching, and psychological dependence to varenicline. However, no serious adverse event was found. When the subjects were classified into the groups with varenicline treatment for less than 4 weeks, 4~8 weeks, and 8 weeks or longer, and were analyzed, the frequency of adverse events was shown to be 5.1% (4 cases), 12.8% (10 cases), and 12.8% (10 cases), respectively, which showed no significant difference among the three groups (p=0.211).
Discussion
Smoking causes cancer, cardiovascular diseases, and pulmonary diseases. However, the onset of these diseases or early death caused by them can be reduced via smoking cessation11-14. Many smokers decide to quit smoking due to reasons such as new year goal or health, but the success rate of smoking cessation by will alone has been reported to be only 3~5%, which is very low15,16. The reasons for that is because of nicotine dependence, a major causative factor of smoking17. Varenicline is a partial agonist of nicotine receptors, and is currently used as the most effective smoking cessation aid that reduces smoking desire and withdrawal symptoms9,18-22. However, due to drug cost, adverse events, and drug incompliance in Korea, 12-week varenicline treatment is rarely conducted23. Song et al.23 reported that smoking cessation subjects who completed 12-week varenicline treatment accounted for 7.7%, and their success rate of 6-month smoking cessation was 35.4%. A univariate analysis showed that factors related to 6-month smoking cessation success were nicotine dependence, mean daily smoking amount, weekly drinking amount, varenicline treatment duration, number of outpatient visit, and reasons for visiting, whereas a multivariate analysis showed that factors related to 6-month smoking cessation success were mean daily smoking amount, varenicline treatment duration, and reasons for visiting the clinic. When the aforementioned results were compared with the results this study, they were similar in that the success rate of smoking cessation increased in the cases of older age at the time of visiting the smoking cessation clinic, more frequent outpatient visit, longer varenicline treatment duration, and underlying diseases. However, in this study, the success rate of 6-month smoking cessation was 47.4%, which was irrelevant to the mean daily smoking amount, number of drinking, and nicotine dependency. Twenty-eight percent of the subjects who received varenicline completed 12-week varenicline treatment, and their success rate of 6-month smoking cessation was 64%, which was higher than 41% of the group that early terminated varenicline treatment. Considering that the subjects of this study were males in their 40~50s (74%) with high education (84%) and high income (85%) from a socioeconomic point of view, it is likely that compared to smokers in their 20~30s who have relatively lower financial security and less interest in health, the success rate of 6-month smoking cessation was higher in the subjects of this study due to more experiences in abnormal symptoms and signs, increased interest in health, and stronger motivation for smoking cessation as a required behavior. In addition, although the presence of underlying diseases was a factor related to 6-month smoking cessation success, no significant difference was found when the subjects were classified into the subgroups by disease, and then analyzed. Thus, a further study is required to be conducted on a larger number of subjects.
A further systematic study is required for reasons for the early termination of varenicline treatment. One thing that should be noted in this study is that the odds ratio of 6-month smoking cessation success increased as varenicline was treated one more week although the treatment period did not reach 12 weeks, the recommended period of varenicline treatment. Thus, it is important to increase drug compliance for varenicline treatment unless a particular contraindication is commented in a smoking cessation consultation. Adverse events were observed in approximately 30% of the subjects who received varenicline, but most of them were mild gastrointestinal symptoms. In the case of nausea, the symptom was improved as time passed by even if varenicline dose was constantly maintained, and it was resolved if varenicline dose decreased. Thus, this symptom can be controlled if an education on the efficacy and adverse events of varenicline is provided to smokers upon treatment. If varenicline is covered by medical insurance, thereby saving the cost of varenicline treatment, patient's drug compliance could be improved.
This is a retrospective observatory study that was conducted on middle-aged male subjects with relatively high educational background and high income, who underwent a medical examination in a single institution. Although the result of this study is hard to be generalized and applied to the Korean male smoker population, an effort to improve drug compliance for varenicline in clinical practices could be helpful for the long-term success of smoking cessation.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






