



Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by airway inflammation, parenchymal destruction, and expiratory airflow limitation [1]. It causes various respiratory symptoms such as cough, sputum, and dyspnea on exertion. However, the manifestation of COPD is usually not limited to the respiratory system. It may present with various systemic manifestations such as cardiovascular disease, osteoporosis, mental health issue, malnutrition, and skeletal muscle dysfunction [2]. These respiratory and systemic manifestations might decrease the quality of life (QOL) and cause psychological problems in COPD patients. For example, depression is a frequent comorbidity, occurring in 15% to 40% of COPD patients [3-5]. In addition, metabolic syndrome is more frequently found in patients with COPD, with an estimated prevalence of more than 30% [6,7].
Alcohol consumption may affect QOL and depressive mood in the general population. In a cross-sectional study in Finland, the amount of alcohol drinking and frequency of binge drinking were associated with impaired QOL in persons with depression [8]. Contrarily, moderate-risk alcohol drinkers had a lower risk of depressive mood and higher QOL than low-risk drinkers in the general population in Korea [9]. A cohort study in Korea has reported that as a metabolic syndrome-related factor, heavy alcohol drinking is associated with higher blood pressure (BP), fasting glucose, and triglyceride (TG) levels in the general population [10].
People with COPD usually stop smoking because of respiratory symptoms or a doctorŌĆÖs advice. However, many continue to drink to reduce psychological stress and halt the declining QOL after quitting smoking. Relationships of alcohol consumption with QOL, depressive mood, and metabolic syndrome-related factors have not been extensively studied in patients with COPD. Therefore, the objective of this study was to investigate whether alcohol consumption might be associated with QOL, depressive mood, and metabolic syndrome in patients with COPD.
Materials and Methods
1. Study population
This was designed as a cross-sectional observational study. Data were obtained from the Korea National Health and Nutrition Examination Survey from 2014 and 2016 (KNHANES VI). KNHANES is a nationwide, population-based, cross-sectional program that collects detailed information on the health and nutrition status of non-institutionalized Korean population. Data on demographics, smoking status, and physician-diagnosed comorbidities such as hypertension, stroke, ischemic heart disease, diabetes mellitus, activity limitations, lung function, depressive mood, and QOL were obtained using complex, stratified, multistage probability sampling to represent the Korean population.
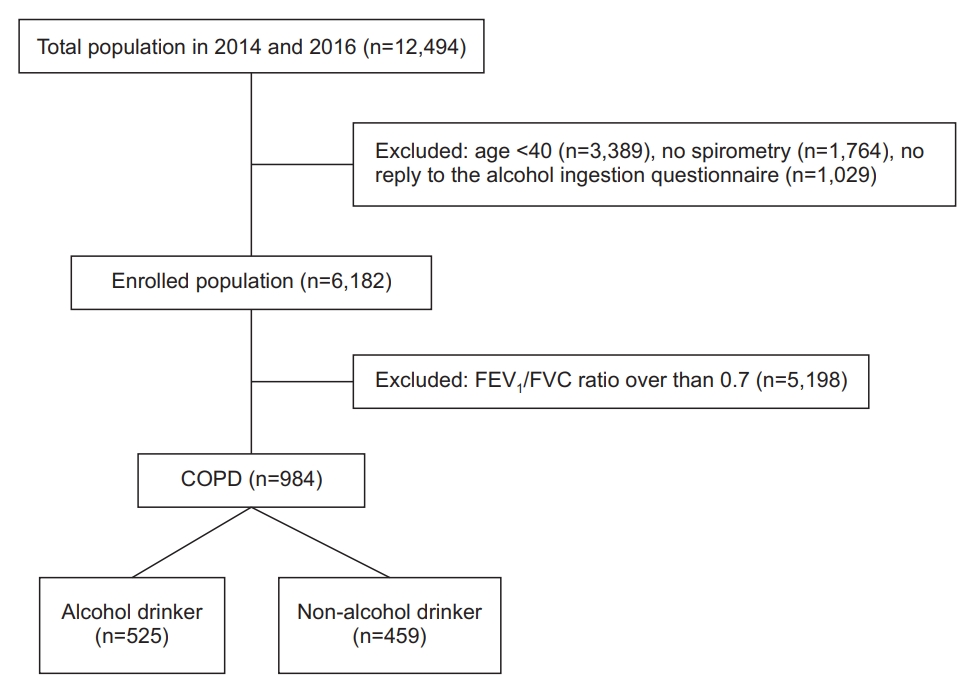
Of a total of 12,494 participants in 2014 and 2016 of the KNHANES, we included adults aged over 40 years who had received pulmonary function tests. We also included participants who replied to the alcohol ingestion questionnaire (Figure 1). The Institutional Review Board (IRB approval number: 2013-07CON-03-4C, 2013-12EXP-03-5C, and 2018-01-03-PA) approved the KNHANES protocol of the Korean Centers for Disease Control and Prevention. All participants provided informed consent to participate in this study.
2. Definition of obstructive lung disease
The presence of obstructive lung disease (OLD) was defined as forced expiratory volume in 1 second (FEV1) divided by forced vital capacity (FVC) Ōēż0.7 as suggested by the Global Obstructive Lung Disease (GOLD) guidelines. Trained medical technicians conducted pulmonary function tests using the Thoracic Society/European Respiratory Society Task Force with dry rolling seal spirometers (Model 2130, Sensor Medics, Yorba Linda, CA, USA).
3. Assessment of QOL and depressive mood
Patient Health Questionnaire-9 (PHQ-9) is a screening tool for measuring depressive mood. It comprises nine symptom-related items that measure the frequency of a participantŌĆÖs experience of depressive symptoms over the previous 2 weeks. Participants responded to each item with ŌĆ£not at allŌĆØ (scored as 0), ŌĆ£on several daysŌĆØ (scored as 1), ŌĆ£on more than half the daysŌĆØ (scored as 2), or ŌĆ£nearly every dayŌĆØ (scored as 3). Scores for all individual items were summed to obtain a total PHQ-9 score ranging from 0 to 27, with a higher score indicating a higher severity of depressive mood.
The European Quality of Life Questionnaire-5D (EQ-5D) was used to evaluate five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) to assess QOL. Participants responded to each dimension with three functional levels: no problems, some problems, or extreme problems. These responses were converted into EQ-5D summary index scores using a specific Korean valuation set developed by the time trade-off protocol at the Korean Centers for Disease Control and Prevention. EQ-5D index ranged from 0 to 1 [11].
4. Assessment of metabolic syndrome
Metabolic syndrome was defined according to the new International Diabetes Federation criteria except that waist circumference cutoff was modified to be specific to the Korean population [12]. According to these criteria, metabolic syndrome was defined based on central obesity, waist circumference Ōēź90 cm in men and Ōēź80 cm in women, or a body mass index (BMI) Ōēź25 kg/m2, and any two of the following four factors: (1) systolic BP Ōēź130 mm Hg, diastolic BP Ōēź85 mm Hg, or use of antihypertensive medications; (2) TG level Ōēź150 mg/dL or use of anti-hyperlipidemic medications; (3) high-density lipoprotein cholesterol (HDL-C) level <40 mg/dL in men and <50 mg/dL in women; and (4) fasting plasma glucose level Ōēź100 mg/dL or previous diagnosis of diabetes.
5. Assessment of alcohol consumption
The definition of a drinker was based on self-report. A person was classified as a drinker if he or she had consumed at least one glass of alcohol per month over the past year without distinguishing between beers, soju, and foreign liquors. Otherwise the person was classified as a non-drinker. Alcohol drinkers were additionally asked to complete a questionnaire regarding the amount and frequency of alcohol consumption in the past 30 days. Daily alcohol consumption was calculated based on the average consumption frequency and amount per occasion. Participants were categorized into three groups according to their baseline alcohol consumption: low-risk (<5 g/day), moderate-risk (Ōēź5 but <30 g/day for men, Ōēź5 but <15 g/day for women), and high-risk (Ōēź30 g/day for men, Ōēź15 g/day for women) alcohol drinkers [13].
6. Nutrition survey
The nutrition survey was divided into a 24-hour dietary recall, a dietary behavior survey, and a food security survey. For the 24-hour dietary recall, a team of dieticians visited each participantŌĆÖs household and conducted individual interviews with all household members over the age of 1 year to collect data about names of dishes or food, amounts consumed, and the location and type of meals eaten a day prior in chronological order. To determine the exact amount of the intake, we investigated each individualŌĆÖs intake using various measuring aids. For nutrients, we examined total energy and proportions of energy from carbohydrates, proteins, fats, and other components [14].
7. Statistical analysis
All continuous values are described as mean┬▒standard deviation and categorical values are reported as absolute numbers and percentages. StudentŌĆÖs t-test or Mann-Whitney U test was used to analyze continuous values according to data distribution. Categorical values were analyzed using the chi-square test or FisherŌĆÖs exact test. Multiple logistic regression analysis was performed to evaluate factors associated with depressive mood and QOL. In all comparisons, a p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA) for Windows (Microsoft Corporation, Redmond, WA, USA).
Results
1. Baseline characteristics of alcohol drinkers and non-drinkers
A total of 984 participants with OLD (695 males, 289 females, age 65.8┬▒9.7 years) were enrolled in the study. A total of 525 alcohol drinkers and 459 non-alcohol drinkers were identified (Figure 1). Alcohol drinkers were younger than non-alcohol drinkers. Proportions of males and current smokers were higher in alcohol drinkers than in non-alcohol drinkers. Non-alcohol drinkers also had worse lung functions as assessed by FEV1, FVC, and FEV1/FVC ratio than alcohol drinkers. Regarding comorbid illnesses, they showed no significant difference between the two groups. Sputum production over 3 months was significantly higher in alcohol drinkers than in non-alcohol drinkers (14.3% vs. 5.5%). Nutritional intakes such as water, protein, lipid, and whole food were significantly higher in alcohol drinkers than in non-alcohol drinkers. In laboratory findings, serum glucose, aspartate transaminase, alanine transferase, hemoglobin, and hematocrit levels were significantly higher in alcohol drinkers than in non-alcohol drinkers (Table 1).
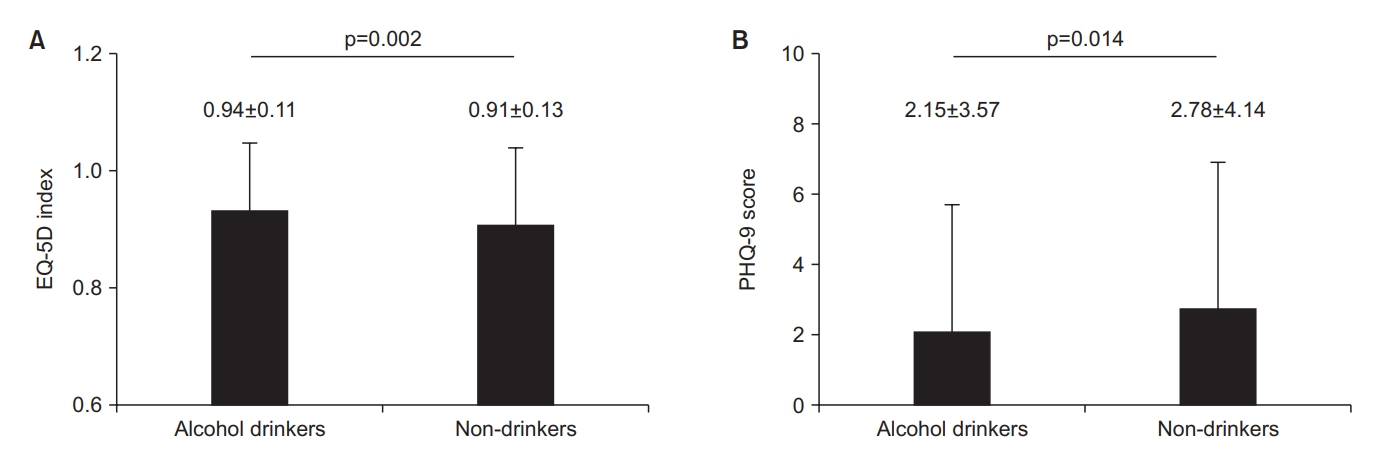
2. Comparison of QOL (EQ-5D index) and depressive mood (PHQ-9 score) between alcohol drinkers and non-alcohol drinkers in OLD patients
The EQ-5D index was significantly higher in alcohol drinkers than in non-alcohol drinkers (0.94┬▒0.11 vs. 0.91┬▒0.13, p=0.002). PHQ-9 scores were considerably lower in alcohol drinkers than in non-alcohol drinkers (2.15┬▒3.57 vs. 2.78┬▒4.13, p=0.014) (Figure 2). Among alcohol drinkers, PHQ-9 scores were significantly higher in high-risk alcohol drinkers than in light to moderate-risk alcohol drinkers (2.64┬▒4.19 vs. 1.83┬▒3.08, p=0.01). However, there were no significant differences in EQ-5D index score between high-risk alcohol drinkers and light to moderate-risk alcohol drinkers (0.94┬▒0.1 vs. 0.93┬▒0.12, p=0.342) (Table 2).
3. Factors associated with QOL (EQ-5D index) and depressive mood (PHQ-9 score) in OLD patients
Multiple logistic regression analysis evaluated factors associated with QOL (EQ-5D index) and depressive mood (PHQ-9 score) in OLD. Results showed that QOL, age, male sex, current smoking, activity limitation, sputum production for 3 months, and calorie intake per day were significantly associated with the EQ-5D index. Male sex, BMI, activity limitation, and sputum production were considerably associated with the PHQ-9 score. However, alcohol consumption was not associated with the EQ-5D index or PHQ-9 score (Table 3).
4. Comparison of metabolic syndrome-related factors between alcohol drinkers and non-alcohol drinkers in OLD patients
Results of assessing metabolic syndrome-related factors with alcohol consumption showed that BMI Ōēź25 kg/m2, TG Ōēź150 mg/dL, HDL-C <40 mg/dL in men and <50 mg/dL in women, and BP Ōēź130/85 mm Hg were significantly more common in alcohol drinkers than in non-alcohol drinkers (p=0.035, p=0.001, p=0.001, and p=0.002, respectively) (Table 4).
Discussion
This study evaluated associations of alcohol consumption with QOL and depressive mood in Korean adults with OLD. Results showed that alcohol consumption did not change the QOL or depressive mood in individuals with OLD. However, it might increase the risk of metabolic syndrome. In addition, high-risk alcohol drinkers showed more depressive moods than low to moderate alcohol drinkers.
Associations of alcohol consumption with QOL and depressive mood in the general population have been reported yet. One study from Korea showed that moderate drinkers (alcohol >28 g/week) exhibited lower depressive mood and higher QOL than non-drinkers and lower drinkers [9]. Another study using KNHANES data showed a higher perception of stress and depressive symptoms in high-risk drinkers than in low-risk drinkers [15]. In other countries such as Finland and the United Kingdom, binge or problematic drinkers have poor mental health such as poor satisfaction with life and high psychological stress [16,17].
In patients with mild to moderate COPD, psychiatric problems and alcohol abuse were more common than in age-matched controls, which might impair QOL [18]. A study predicting poor QOL showed that alcohol abuse and degree of airflow limitation might be associated with poor QOL in COPD patients [19]. In our study, alcohol drinkers among COPD patients also tended to have higher QOL and lower depressive moods. However, for those who were high-risk drinkers, this difference in depressive mood disappeared compared to non-alcohol drinkers. Moreover, the depressive mood was higher in high-risk alcohol drinkers than in low and moderated-risk alcohol drinkers. Therefore, low and modest alcohol consumption might not affect QOL or depressive mood. However, heavy alcohol consumption might be associated with increased depressive mood in COPD patients.
Metabolic syndrome is also commonly considered one of the systemic manifestations of COPD [2]. In one study, over 50% of COPD patients showed metabolic syndrome, which was more than 15% higher than that in BMI-matched healthy controls [20]. A national survey using data from KNHANES showed that the prevalence of metabolic syndrome was significantly higher in individuals with COPD than in those without COPD regardless of gender (33.0% vs. 22.2% in men and 48.5% vs. 29.6% in women) [21].
A cohort study in the general Korean population, including a national nutritional survey, showed that heavy alcohol consumption was associated with a significantly higher ratio of high BP, higher TG and fasting blood glucose lvels, and lower HDL levels [10]. A prospective study in Korea showed that alcohol drinking was associated with the development of metabolic syndrome and that the risk was exacerbated by heavy alcohol consumption [13]. Consequently, alcohol consumption might increase the risk of metabolic syndromes in COPD patients. In our study, alcohol drinkers in the COPD population showed a higher incidence of BMI over 25 kg/m2, higher fasting blood glucose and TG levels, lower HDL levels, and higher BP.
Total calorie intake was associated with a higher QOL in the COPD population in this study. Malnutrition is a common problem in COPD patients. It can lower QOL in COPD patients [22]. Nutritional support such as extra meals might increase the QOL in the COPD population [23]. Therefore, nutritional support might improve QOL in the COPD population.
In this study, sputum production, not cough, was associated with depressive mood and QOL in the COPD population. Several studies have shown that cough and sputum production are essential determinants of QOL in stable COPD patients [24]. A cross-sectional study showed that chronic sputum production could impair the QOL and worsen anxiety and depression, which was more in women than in men, regardless of lung function [25]. Findings in this study were consistent with those of previous studies. Cough and sputum production were associated with COPD exacerbation risk in previous studies [26,27], which might be associated with higher depressive mood and lower QOL in the COPD population [28].
This study has some limitations. First, our data did not include any post-bronchodilator spirometer measurement. In addition, the diagnosis of COPD was assessed only based on pre-bronchodilator spirometer measurement. Second, men had a higher proportion than women among alcohol drinkers and vice versa. Differences in male to female ratio might affect BMI. In a Korean study investigating the prevalence of metabolic syndrome between males and females, metabolic syndrome was found to be more common in older women than in middle-aged men [29]. Third, COPD patients usually have a high prevalence of depression. However, overall PHQ-9 scores were relatively lower in this study. This might be due to this studyŌĆÖs cross-sectional design and the fact that the diagnosis of COPD was assessed by spirometric criteria. A prospective evaluation might be required to assess alcohol consumption and depressive mood in patients with COPD in the future.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






