Normalization of Elevated CA 19-9 Level after Treatment in a Patient with the Nodular Bronchiectatic Form of Mycobacterium abscessus Lung Disease
Article information
Abstract
Carbohydrate antigen 19-9 (CA 19-9) is a widely-used tumor marker in patients with pancreatic cancer. However, some patients with respiratory disease also exhibit elevated serum CA 19-9 levels. We report a case of normalization of elevated serum CA 19-9 levels after treatment of the nodular bronchiectatic form of Mycobacterium ab scessus lung disease. A 40-year-old man visited our hospital because of chronic cough and sputum. A computed tomography scan revealed severe bronchiectasis in the right upper and right middle lobes. Nontuberculous mycobacteria were repeatedly isolated and identified as M. abscessus. The serum CA 19-9 level was elevated to 142.35 U/mL (normal range, <37 U/mL). Surgical resection was performed because of failure of sputum conversion after antibiotic treatment. The serum CA 19-9 level returned to the normal range after surgery. This case suggested that serum CA 19-9 levels could be elevated in patients with the nodular bronchiectatic form of M. abscessus lung disease.
Introduction
Serum carbohydrate antigen 19-9 (CA 19-9) is a tumor marker that is expressed in tissue as a monosialoganglioside and a mucous protein1. It is the most important tumor marker for the diagnosis of pancreatic cancer, and it has become the standard for predicting recurrence of pancreatic carcinoma during follow-up2. However, it can also be elevated in several benign respiratory diseases3. We report a case of normalization of elevated serum CA 19-9 levels after treatment of the nodular bronchiectatic form of Mycobacterium abscessus lung disease.
Case Report
A 40-year-old man was referred to our hospital because of chronic cough and sputum. He had been healthy until five years earlier, when cough and sputum developed. He had no history of pulmonary tuberculosis. The patient had no smoking history or other medical history. He appeared relatively healthy, and no signs of fever, chills, weight loss, or digestive symptoms were observed at the time of visit. He was suffering from productive cough, purulent sputum, and right pleuritic pain. His blood pressure was 134/90 mm Hg, pulse rate 78/min, respiratory rate 20/min, and body temperature 36.1℃. Bronchial breathing sound with inspiratory rhonchi was auscultated on the right upper lung field in the thoracic examination. Laboratory results, including immunoglobulin levels, were normal with the exception of elevated serum CA 19-9 to 142.35 U/mL (normal range, <37 U/mL). Pancreas computed tomography (CT) yielded no specific abnormal findings.
Chest radiography revealed cystic changes in the right upper and middle lung zones. A chest CT scan revealed severe bronchiectasis in the right upper lobe and right middle lobe (Figure 1). There was no evidence of cystic fibrosis or other common causes of bronchiectasis. A sputum Gram stain shows normal flora and routine bacterial culture reveals no pathogens. Numerous acid-fast bacilli were seen in multiple sputum specimens (4+). Nontuberculous mycobacteria were isolated repeatedly from three expectorated sputum specimens and all isolates were identified as M. abscessus by a polymerase chain reaction-restriction fragment length polymorphism method based on rpoB and sequence analysis targeting the rpoB and hsp65 genes4. Drug susceptibility testing was performed at the Korean Institute of Tuberculosis by using a broth microdilution method. The isolated M. abscessus was susceptible to amikacin, cefoxitin, clarithromycin, and ciprofloxacin, but resistant to doxycyline.
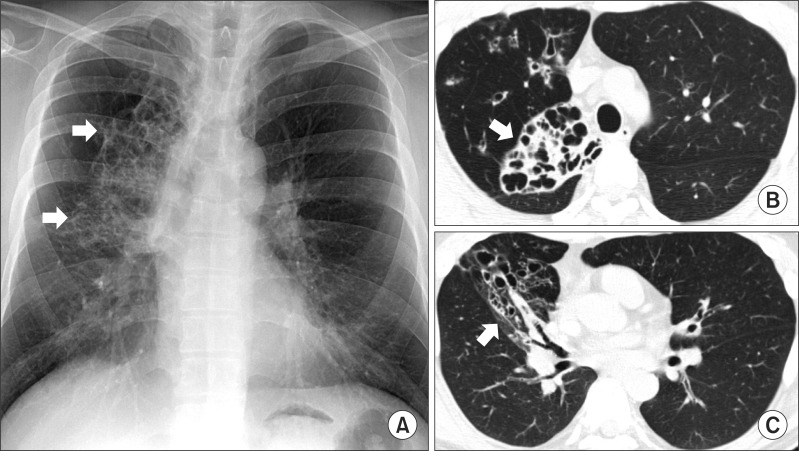
A 40-year-old man with bronchiectasis and nontuberculous mycobacterial lung disease caused by Mycobacterium abscessus. (A) Chest radiography reveals cystic change in the right upper and middle lobes (white arrows). (B) A transverse chest computed tomography (CT) scan (2.5-mm-section thickness) shows total atelectasis and severe bronchiectasis in the right upper lobe (white arrow). (C) A chest CT scan shows bronchiectasis in the right middle lobe (white arrow).
The patient was diagnosed with M. abscessus lung disease, according to the diagnostic guidelines5, and began antibiotic therapy with a two-drug oral regimen that included clarithromycin (1,000 mg/day) and ciprofloxacin (1,000 mg/day), along with an initial 4-week course of amikacin (15 mg/kg/day in two divided doses) and cefoxitin (200 mg/kg/day, maximum 12 g/day in three divided doses)6. Right upper and middle lobectomy was performed because sputum culture was persistently positive after 5 months of antibiotic treatment. Pathologic examinations showed severe bronchiectasis and associated chronic granulomatous inflammation with caseous necrosis. Antibiotics were continued 12 months after surgery. Negative sputum culture conversion was achieved immediately after surgery and was maintained until the completion of antibiotic treatment. The serum CA 19-9 levels returned to the normal range (13.56 U/mL) 1 month after surgery and remained within the normal range (15.51 U/mL) 12 months after surgery (Figure 2).
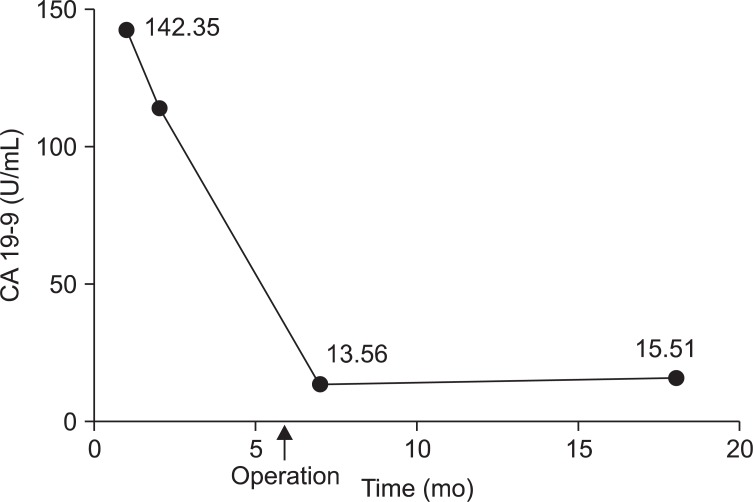
Changes in serum carbohydrate antigen 19-9 (CA 19-9) level. At the time of diagnosis with Mycobacterium abscessus lung disease, serum CA 19-9 level was elevated to 142.35 U/mL. It returned to the normal range (13.56 U/mL) after surgery (black arrow) and remained up to 12 months later.
Discussion
Although CA 19-9 is a well-known tumor marker for pancreatic cancer, increased levels of CA 19-9 can also be detected in several benign conditions. Investigators have reported elevated serum levels of CA 19-9 in patients with nonmalignant respiratory diseases, such as diffuse panbronchiolitis and bronchiectasis7,8. In addition, a recent case-control study in Korea demonstrated that bronchiectasis, bronchiolitis, emphysema, and interstitial fibrosis were independent risk factors for increased CA 19-9 concentrations9. To our knowledge, this is the first documented case in which elevated serum CA 19-9 levels were normalized after treatment of the nodular bronchiectatic form of M. abscessus lung disease.
In previous studies that used immunohistochemical staining, CA 19-9 was reported to be selectively expressed in regenerating epithelial cells associated with inflammatory changes in the peripheral lungs in patients with idiopathic interstitial pneumonia and diffuse panbronchiolitis, regardless of the etiology7,10. This indicates that the high serum CA 19-9 was probably due to hypersecretion of mucus glycoprotein from hypertrophic glands and/or epithelial cells in the bronchioles. The extravasation into the circulatory system was caused by pathogenic changes accompanying chronic inflammation of the small airways. In this case, the source of the elevated serum CA 19-9 was considered to be the extensive bronchiectasis in the right upper and middle lobes, and chronic inflammation due to M. abscessus lung disease.
Yamazaki et al.11 suggested that serum CA 19-9 represents the activity of Mycobacterium avium lung disease. Bulut et al.12 reported that CA 19-9 and CA 125 increased in relation to the severity of chronic obstructive pulmonary disease. However, further study of the association of disease activity with this tumor marker in nonmalignant respiratory disease is required.
In conclusion, serum CA 19-9 level, which is used as a tumor marker in gastrointestinal cancers, is also elevated in some patients with nonmalignant respiratory diseases. This case suggested that serum CA 19-9 levels could be elevated in patients with the nodular bronchiectatic form of M. abscessus lung disease.
Acknowledgements
This work was supported by the Mid-career Researcher Program through a National Research Foundation grant funded by the Ministry of Education, Science and Technology (2011-0015546).