Multidrug-Resistant Tuberculosis Presenting as Miliary Tuberculosis without Immune Suppression: A Case Diagnosed Rapidly with the Genotypic Line Probe Assay Method
Article information
Abstract
Miliary tuberculosis (TB) is a rare extrapulmonary form of TB, and there have been only two reports of miliary TB associated with infection with multidrug-resistant (MDR)-TB pathogen in an immunocompetent host. A 32-year-old woman was referred to our hospital because of abnormal findings on chest X-ray. The patient was diagnosed with MDR-TB by a line probe assay and was administered proper antituberculous drugs. After eight weeks, a solid-media drug sensitivity test revealed that the pathogen was resistant to ethambutol and streptomycin in addition to isoniazid and rifampicin. The patient was then treated with effective antituberculous drugs without delay after diagnosis of MDR-TB. To the best of our knowledge, this is the first case of miliary TB caused by MDR-TB pathogen in Korea.
Introduction
Although global cooperative efforts have been made to reduce the global incidence of drug-susceptible tuberculosis (TB), multidrug-resistant (MDR)-TB has emerged worldwide over the past 20 years1,2,3. Miliary TB is a clinically rare form of TB and data from the US Centers for Disease Control and Prevention in 2010 indicated that less than 2% of all cases of TB were classified as miliary TB4.
There are several reports of miliary TB caused by MDR-TB pathogen in immunocompromised hosts such as people with acquired immunodeficiency syndrome or on infliximab therapy5,6, but there are only two previous reports of miliary TB caused by MDR-TB pathogen in an immunocompetent host7,8.
Here, we report a documented case of MDR-TB presenting as miliary TB in an immunocompetent patient. This case was rapidly diagnosed as MDR-TB by the molecular reverse hybridization-based line probe assay (LPA) genotypic method, meaning that the patient was administered appropriately modified effective antituberculous drugs without delay. We wish to emphasize the possibility of MDR-TB even in an immunocompetent patient with miliary TB in circumstances where moderate levels of resistance in the TB patient population would be predicted.
Case Report
In May 2013, a 32-year-old woman was referred to our hospital because of abnormal findings on a chest X-ray. She had been healthy until one month before, when a cough and intermittent chills developed. She was a current smoker but denied use of illicit drugs or other relevant medical history.
She had no familial history of TB and denied a contact with a person with TB infection. She acted with a touring company for five years. On examination, she appeared well. Her body weight was 69 kg, height 168.2 cm, temperature 36.2℃, blood pressure 123/80 mm Hg, pulse 78 beats per minute, and oxygen saturation 100% while breathing ambient air. Laboratory results were normal. A human immunodeficiency virus antibody test was negative.
A chest radiograph and computed tomography scan of the chest revealed uniform-sized small nodules randomly distributed throughout both lungs (Figure 1). We performed bronchoalveolar lavage (BAL) and transbronchial lung biopsy at the anterior segment of the right upper lung.
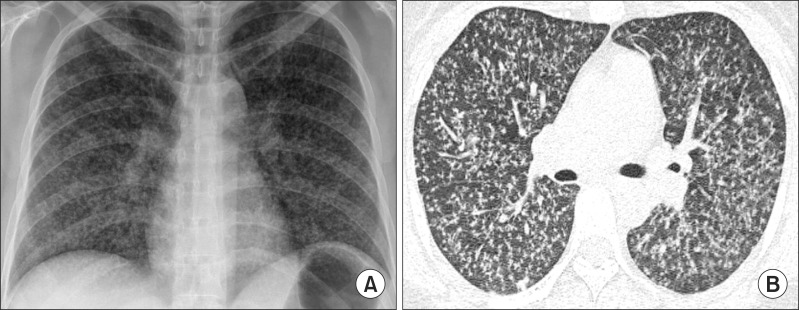
A 32-year-old woman diagnosed as military tuberculosis caused by multidrug-resistant pathogen. (A) Chest radiograph at the time of presentation showed diffuse micro-nodules involving both lung fields. (B) High-resolution computed tomography image (1.0 mm section thickness) revealed uniform-sized small nodules randomly distributed throughout both lungs.
The next day, the microbiological investigation of BAL fluid by TB polymerase chain reaction gave a positive result. We therefore diagnosed the patient with miliary TB and treated her with isoniazid, rifampicin, ethambutol, and pyrazinamide. She was discharged without complication. Two weeks after bronchoscopy, Mycobacterium tuberculosis was isolated from the liquid media of the BAL specimen. We then performed a reverse hybridization-based LPA and a solid-media drug sensitivity test (DST). The patient complained of myalgia and chills for two weeks.
One day later, the LPA revealed that the pathogen had mutations in the katG and rpoB genes (Figure 2), so the patient was suspected to have miliary TB caused by MDR-TB pathogen. Her antituberculous treatment was changed to ethambutol, pyrazinamide, kanamycin, moxifloxacin, prothionamide, and cycloserine. A solid-media DST performed in the Korean Institute of TB using the absolute concentration method was consistent with MDR-TB eight weeks after the isolation of Mycobacterium tuberculosis from the BAL. The solid-media DST report was delayed because of contamination of the specimen. It showed the pathogen to be resistant to ethambutol and streptomycin in addition to isoniazid and rifampicin.
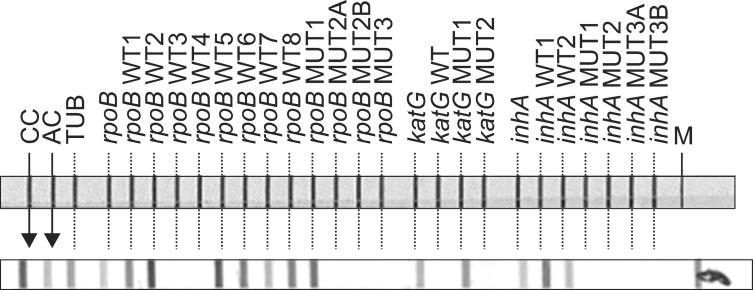
Line probe assay results: for rifampicin, the strain revealed negative results of rpoB WT3 and WT4 probes, and positive result of rpoB MUT1 probe for D516V mutation; for isoniazid, there were missing band of katG WT and additional positive band in katG MUT1 for S315T1 mutation.
Finally, the patient was diagnosed with miliary TB caused by MDR-TB pathogen. Her antituberculous therapy has been maintained with the regimen described above with the exception of ethambutol. Three months after beginning treatment for miliary TB, the patient did not complain of any symptoms and the follow-up chest plain X-ray showed that the disease had partially resolved compared with the initial presentation (Figure 3).

A chest radiography after treatment showed resolution of diffuse micro-nodules involving both lung fields.
Discussion
The overall incidence of TB has been reported to be slowly decreasing since 2004 through the World Health Organization (WHO) Stop TB Strategy, but there is no definitive evidence that the incidence of MDR-TB is decreasing despite this global effort1,3. Despite great efforts in several countries including South Korea that have led to a slow decrease in the overall incidence of TB, surveillance indicates that the incidence of MDR-TB is rising9. Moreover, prevalence of MDR-TB may be suggested three times greater than incidence because MDR-TB patients often live for several years before succumbing to the disease3.
It is known that a number of risk factors for MDR-TB have been critical in the emergence. Almost all are related to poorly functioning National Tuberculosis Program. Other important risk factors are associated with the supply or quality of the drugs, the possible inadequate drug intake by patients, and others, such as the influence of the private sector, deficient infection control in health centers and hospitals, and the possible high prevalence of highly virulent MDR-TB strains of M. tuberculosis. Many other risk factors for MDR-TB have been also identified: previous TB treatment, irregular treatment, female sex, non-permanent residents, urban migration, urban residence, frequent travelers, younger age, lack of a sewage system in the home, alcoholism plus smoking, and lung cavities10. In our case, the patient was only associated with female sex, urban residence, and young age of risk factors for MDR-TB. We repeatedly performed a human immunodeficiency virus antibody test and peripheral CD4/CD8 ratio but the result was unremarkable.
MDR-TB can also cause miliary TB, but the incidence of MDR-TB in miliary TB infection is completely unknown because of the low incidence of this rare extrapulmonary form of TB6,7,11. There have been several case reports of miliary TB caused by MDR-TB pathogen in an immunocompromised host, but only two reports in an immunocompetent host5,6,7. The reason for the high incidence of miliary TB in immunocompromised patients is thought to be the combination of an inadequate immune response and a lack of effective antituberculous treatment.
It is known that in 30% to 65% of cases, microbiological confirmation of miliary TB is on the basis of culture of the pathogen from a respiratory specimen12. In this case, we could detect MDR-TB more rapidly using a molecular (genotypic) method than using conventional (phenotypic) methods such as solid- and liquid-media DST, so we could administer adequate and effective antituberculous treatment without delay. The reverse hybridization-based LPA has been developed for direct detection of MDR-TB strains in clinical specimens. The GenoType MTBDRplus (Hain Lifescience, Nehren, Germany) assay detects MDR-TB by simultaneously detecting mutations in hot spot regions of the rpoB gene to indicate rifampicin resistance and mutations in katG315 and inhA regulatory regions to indicate isoniazid resistance13. The LPA has performed satisfactorily in several clinical settings for detection of MDR-TB in clinical samples13,14,15. Therefore, it can be considered that a rapid genetic DST such as the LPA is a suitable alternative method for early detection of MDR-TB in miliary TB.
In conclusion, the possibility of MDR-TB should be considered in miliary TB despite its rarity, especially in regions such as Korea with moderate levels of drug resistance among TB patients. In addition, a molecular DST such as the LPA can be a good method to diagnose MDR-TB more rapidly in cases of extrapulmonary TB infection such as miliary TB. To the best of our knowledge, this is the first documented case of miliary TB caused by MDR-TB pathogen in Korea.
Notes
No potential conflict of interest relevant to this article was reported.