


Introduction
Cancer is a disease of the cellular genome, and therefore lung cancers are understandably characterized by abundant genetic diversity. Information about genetic alterations and protein expression level is considered alongside histology in order to better comprehend the pathogenesis of lung cancer1. Recent advances in the field of molecular-based cancer biology revealed that approximately 60% of adenocarcinomas and 20% of squamous cell carcinomas have an identified gene signature, and a finding that has led to the successful development and approval of targeted therapies2. The use of targeted agents in lung cancer patients harboring epidermal growth factor receptor (EGFR) gene mutations or anaplastic lymphoma kinase (ALK) gene rearrangements has been associated with dramatic response rates and improved progression-free survival (PFS)3,4,5,6,7, therefore, molecular testing is now routinely used to guide clinical care of lung cancer patients to predict one's therapeutic response1.
Moreover, as the technology and knowledge supporting molecular testing is rapidly evolving, the landscape of targetable genomic alterations in lung cancer is expanding2,8,9,10,11. However, the challenge of identifying biologically relevant driver mutations from the vast majority of passenger mutations remains.
To date, introduction of next-generation sequencing (NGS) technology offers the ability to detect high-throughput, multiple genetic alterations in both constitutional and cancer genomes12. Such modern, but costly, technologies have not only contributed to our understanding of lung cancer biology, but have also provided the impetus for technical advances that may improve our ability to accurately discover the cancer genome13,14.
This article will summarize the current state of the most commonly altered and most clinically relevant genes in lung cancer and potential future developments in molecular testing of lung cancer will be briefly reviewed.
Current Status
1. Novel molecular targets
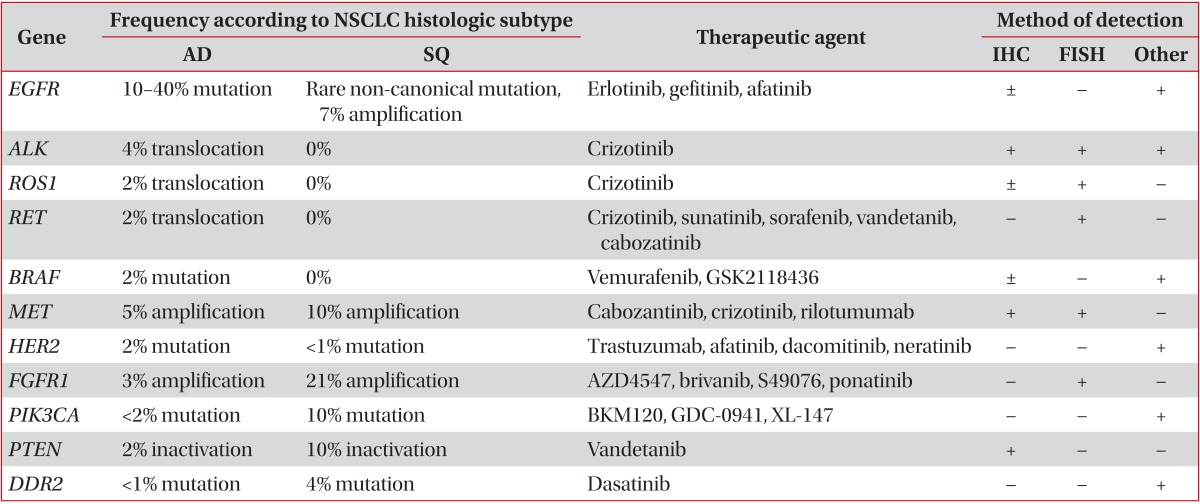
Although EGFR mutations and ALK fusions are well-characterized molecular targets in non-small cell lung cancer (NSCLC), activating alterations in a variety of potential oncogeneic driver genes have also been identified in NSCLC. Table 1 summarizes a variety of genes involved in targeted treatment of NSCLC along with their respective histologic subtypes and the method of detection. However, it is important to recognize that not all potentially targetable biomarkers have been standardized outside of clinical trials. A deeper understanding of the molecular alteration of lung cancer may ultimately lead to personalized treatment strategies, which will improve care for those patients most likely to benefit, and spare the cost and morbidity associated with failed treatment interventions.
1) EGFR
EGFR encodes a transmembrane tyrosine kinase with an extracellular ligand-binding domain and an intracellular tyrosine kinase domain15. Activating somatic mutations are present in exons 18-21 of the tyrosine-kinase domain and deletions in exon 19 and the L858R point mutation in exon 21 occur in 90% of all EGFR mutations. They are associated with a response rate of approximately 70% to EGFR-tyrosine kinase inhibitor (TKI) therapy16. EGFR mutations are primarily seen in adenocarcinoma. Therefore, EGFR mutation analysis is the best predictive marker for the use of EGFR-TKI therapy in NSCLC with an adenocarcinoma component, but gender, ethnicity, and smoking status are unsuitable for use as triage for mutation analysis. The most common mechanism of resistance to EGFR-TKI is the T790M gatekeeper mutation, caused by a single-base substitution of C to T, at nucleotide 236917.
2) ALK
The rearrangement results from a short inversion in chromosome 2p, whereby ALK signaling is activated by the creation of oncogenic fusions of the intron 10 of ALK gene within an upstream partner intron 13 of echinoderm microtubule associated protein-like 4 (EML4)6. More recently, less than 1% of ALK rearrangements cases have different partner genes including kinesin family member 5B (KIF5B), TFG, and KLC-111,18. ALK rearrangements occur in approximately 4% of lung adenocarcinoma patients, usually young, non-smokers with clinically advanced disease6,7,8. The United States Food and Drug Administration approved the ALK Break Apart fluorescence in situ hybridization (FISH) Probe Kit (Abbott Molecular, Des Plaines, IL, USA) as a companion diagnostic for targeted therapy with crizotinib in lung cancers1.
3) ROS1
ROS1 is a proto-oncogene located on chromosome 6q22 that encodes a transmembrane tyrosine kinase receptor of the insulin receptor family19. ROS1 gene rearrangements are known oncogenic drivers in NSCLC, and several fusion partners have been identified, including CD74, SLC34A2/NaPi2b, and FIG9,19. ROS1 fusions are present in about 2% of NSCLC cases and are often seen in young, non-smokers with adenocarcinoma, a population similar to those with ALK-rearranged NSCLC9,19. There is in vitro and early clinical evidence that lung cancers with ROS1 rearrangements are sensitive to TKIs including crizotinib9,11,19.
4) RET
RET is a proto-oncogene located on chromosome 10q11.2 that encodes a receptor tyrosine kinase involved in neural crest development20. Translocations resulting in fusions with several partners have been reported in lung cancer, including multiple variants of KIF5B-RET (the most common type), CCDC6-RET (PTC1), NCOA4-RET (PTC3), and TRIM33-RET2. RET fusions are known to occur in the young, non-smokers with adenocarcinoma, but no other driver mutations, and can be targeted with TKIs such as sunitinib, sorafenib, vandetanib, and cabozantinib2,9,11,20.
5) BRAF
BRAF encodes a serine/threonine protein kinase that is the downstream effector protein of KRAS and activates the mitogen-activated protein kinase (MAPK) signal transduction pathway involved in the regulation of cell proliferation and survival11,21. In contrast to melanoma, about 50% of the mutations are non-V600E mutations such as L596R and G468A. It is unknown whether V600E BRAF mutations function as driver mutations and other mutations as passenger mutations2. Non-V600E mutations have been associated with current or former smokers, while V600E mutations appear to be more common in female, non-smokers11,21. BRAF-mutated NSCLC cases have been reported to respond to vermurafinib2,11.
6) MET
MET is a proto-oncogene located on chromosome 7q21-q31 that encodes a transmembrane tyrosine kinase receptor for its ligand hepatocyte growth factor (HGF)22. Mutations in MET are rare, but a high MET gene copy number has been detected in 1-11% of NSCLC cases. High gene copy numbers are more common in squamous cell carcinoma than adenocarcinoma and are often associated with high MET protein expression and poor prognosis9,11. MET amplification that drives and maintains the phosphatidylinositol 3-kinases (PI3K)/AKT pathway, bypassing EGFR blockade by TKIs, has emerged as one of the critical events for secondary resistance to EGFR-TKIs in patients with EGFR-mutated lung adenocarcinoma23. A number of therapeutic agents targeting the MET/HGF pathway are in clinical development, including cabozantinib, crizotinib, and rilotumumab (antagonistc antibodies against HGF)9.
7) HER2
HER2 is member of the HER (EGFR) family of tyrosine kinase receptors. HER2 mutations are detected mainly in exon 20 in approximately 1-2% of NSCLC cases, predominantly in adenocarcinomas in non-smoking women11. HER2-mutated adenocarcinoma cases have been reported to respond to trastuzumab and afatinib24.
8) FGFR1
FGFR1 is a membrane-bound tyrosine-kinase receptor involved in the regulation of cell proliferation and angiogenesis through activation of the MAPK and PI3K pathways9,25. FGFR1 amplification occurs more frequently in squamous cell carcinoma (21%) than in adenocarcinoma (3%)9,25. The novel FGFR inhibitor ponatinib may be effective in patients with FGFR1 overexpression and the results of ongoing trials are pending25.
9) PIK3CA
PI3K protein family are intracellular lipid kinases and the main catalytic subunit, the p110α isoform, is encoded by the PIK3CA9. PIK3CA mutations mostly involve the catalytic domain and have been identified in approximately 1-3% of NSCLCs, particularly in squamous cell carcinomas9,26. Trials with PI3K inhibitors in combination with chemotherapy and other targeted agents are ongoing.
10) PTEN
PTEN encodes a lipid and protein phosphatase on chromosome 10 that plays a significant role in cell cycle progression, apoptosis, growth, proliferation, and migration via negative control of the PI3K/AKT pathway27. PTEN mutations and loss of PTEN protein expression are relatively common in squamous cell carcinoma9. The TKI vandetanib has shown efficacy against EGFR mutation-positive lung cancer cell lines showing a loss of PTEN28.
2. Present strategy for molecular testing
The molecular targets as described above now define the characteristics of NSCLC. However, EGFR mutation testing and ALK rearrangement status are the only two molecular makers considered the standard-of-care of NSCLC treatment in daily practice currently. The development of new therapeutic agents has led accurate histologic subtyping and molecular predictive testing to become mandatory in NSCLC cases.
1) Histologic subtyping
Histologic subtyping is still important in triaging tumor samples for appropriate molecular testing, as pathologists become more important in the management of patients with lung cancer. It has become clinically relevant to distinguish between adenocarcinoma and squamous cell carcinoma, as the chemotherapy regimen differs for these histologic subtypes1. Because minimally invasive procedures must be employed to obtain diagnostic material in more than 85% of NSCLC cases, an accurate but tissue-sparing approach from the limited cytology or small biopsy specimen is necessary1. Pathologists should try to classify further poorly differentiated NSCLC with the application of a panel of immunohistochemical markers, such as thyroid transcription factor-1 and napsin A to identify an adenocarcinoma component, and p63/p40 to identify a squamous cell carcinoma component30.
2) Molecular guidelines for testing of EGFR and ALK
Several guidelines for molecular testing have been published in the past couple of years1,31,32. Recently, the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology guidelines provide the first standardized evidence-based approach for performing molecular testing to on select patients with lung cancer for EGFR or ALK TKI therapy that is multidisciplinary and multicontinental in scope1. The details have been described elsewhere. Briefly, adenocarcinoma is a basis for conducting molecular testing. Specimens from either primary or metastatic lesions are equally suitable for testing. For limited specimens, EGFR testing should be prioritized first and ALK testing should be prioritized second over other molecular markers. The guidelines encourage EGFR and ALK testing of biopsies at the time of diagnosis for patients presenting with early stage lung cancer. Alternatively, if testing is not performed in these early stage cancers, the guidelines encourage the retaining of cancer tissue for future biomarker testing. Mutation analysis, using a validated method with sufficient performance characteristics, such as direct sequencing, pyrosequencing, and peptide nucleic acid polymerase chain reaction (PCR) clamping, is recommended for EGFR mutation testing. A wide range of sample types, including cytology specimens and fixatives (formalin-fixed paraffin-embedded [FFPE], fresh, frozen, and alcohol) are allowable for EGFR mutation testing. FISH assays using dual-labeled break-apart probes are recommended for ALK gene rearrangement testing1.
Future Directions
1. Future development of molecular testing
Advances in genomic technology such as NGS and multiplex PCR assays have now made it possible to analyze the genomic landscape of lung cancer tissues comprehensively. A detailed understanding of the complex genetic pathways responsible for the initiation and maintenance of malignant transformation may lead to the identification of vulnerabilities in cancers, and in turn may enable identification of novel therapeutic targets.
1) NGS
NGS offers simultaneous sequencing of thousands to millions of short nucleic acid sequences in a massively parallel way12. These modern but costly technologies have been applied to whole genome sequencing and whole exome sequencing for the discovery of mutations and polymorphisms, transcriptome sequencing for the quantification of gene expression, small ribonucleic acid sequencing for microRNA profiling, large-scale analysis of DNA methylation, and chromatin immunoprecipitation mapping of DNA-protein interaction. NGS can detect chromosomal rearrangements and gene copy number alterations at a very high resolution33. It can be performed on FFPE and freshly collected tissue specimens and on small fine-needle aspiration biopsies.
Moreover, targeted NGS is beginning to be implemented in clinical laboratory practice. It is applied to detect individual mutations in cancer-related genes that may assist in cancer diagnosis, have prognostic value, or be used for prediction of response to targeted therapy8,13. Targeted NGS assays require no prior knowledge of the mutations present in a patient's tumor and are not limited to an evaluation of comparatively few 'hot spots' in which specific mutations are known to occur13.
However, NGS is not clinically applicable as of today. The implementation of NGS technology in a clinical laboratory is complex and requires significant expertise in clinical, technical, cost-benefit, and the bioinformatics aspects of sequencing. Careful ethical consideration must also be given to the design of control arms in clinical trials of biomarker-selected patients8,9.
2) Multiplex PCR
Multiple PCRs that evaluates known 'hot spot' mutations by multiplex PCR involve the simultaneous amplification of two or more cDNA/DNA targets in a single reaction vessel with uniquely labelled probes for each target34. A number of multiplex PCR-based assays area available, including SNaPshot (Applied BIosystems, Foster City, CA, USA) and Sequenome MassARRAY (Sequenom Inc., San Diego, CA, USA)9. Multiplex PCR has been used to differentiate metastases from synchronous primary tumors in patients with multiple lung masses, and has the advantage of needing only a small sample of tumor compared with conventional tests, but it is restricted to codons previously determined as mutation hotspots, and is unable to detect chromosomal rearrangements or determine gene copy number9.
2. The Cancer Genome Atlas (TCGA) Project
More recently, systematic cancer genomics projects have applied emerging technologies to the analysis of specific tumor types including the TCGA project35. TCGA's principal aims are to generate, quality control, merge, analyze, and interpret molecular profiles at the DNA, RNA, protein, and epigenetic levels for hundreds of clinical tumors from various tumor types and their subtypes35. By the end of 2015, the TCGA Network plans to have achieved the ambitious goal of analyzing the genomic, epigenomic, and gene expression profiles of more than 10,000 specimens from 25 different tumor types including lung cancer. TCGA has already identified both common and unique mutation spectra and pathway activation in 183 lung adenocarcinomas36 and 178 squamous cell carcinomas37, two major histologies in NSCLC. Exonic regions of the 183 adenocarcinoma cases contained 77,736 somatic variants corresponding to a median of 8.1 mutations/megabase (MB) and a mean of 11.9 mutations/MB (range, 0.04-117.4 mutations/MB)36, whereas a total of 48,690 non-silent mutations with a mean of 228 non-silent and 360 total exonic mutations per tumor, corresponding to a mean somatic mutation rate of 8.1 mutations/MB and media of 8.4/MB in squamous cell carcinoma37. Those rates are higher than rates observed in other TCGA projects including acute myelogenous leukemia (0.56/MB), breast carcinoma (1.0/MB), ovarian cancer (2.1/MB), glioblastoma multiforme (2.3/MB), and colorectal carcinoma (3.2/MB).
1) Adenocarcinoma
Statistical driver analysis yielded previously reported and novel lung adenocarcinoma genes and these included lung adenocarcinoma genes with non-synonymous mutation frequencies consistent with previous reports: TP53 (50%), KRAS (27%), EGFR (17%), STK11 (15%), KEAP1 (12%), NF1 (11%), BRAF (8%), and SMAD4 (3%). In total, 25 genes were shown to have a statistically significant number of mutations in lung adenocarcinoma. Unexpectedly, U2AF1, RBM10, and ARID1A mutations were identified. One of the most significantly mutated genes in this lung adenocarcinoma cohort was U2AF1, which had non-synonymous mutations in 3% of cases. U2AF1 mutation may confer tumorigenic capability independent of known proliferations-sustaining driver genes and patients with U2AF1 mutations had significantly reduced PFS. RBM10, encoding an RNA-binding protein, was mutated in 7% of cases and its mutations co-occurred with those in known lung adenocarcinoma oncogenes. ARID1A, encoding a key protein in the SW1/SNF chromatin-remodeling complex, was mutated in 8% of cases and showed a significant accumulation of nonsense substitutions and frameshift indels36.
2) Squamous cell carcinoma
Lung squamous cell carcinoma is characterized by complex genomic alterations. In total, 18 genes were shown to have a statistically significant number of mutations including mutation of TP53 in nearly all specimens. Significantly altered pathways by mutation or somatic copy number alterations included NFE2L2/KEAP1 in 34%, SOX2/TP63/NOTCH1 pathways in 44%, one of three components of the PI3K/AKT pathway (PIK3CA, PTEN or AKT3) in 47%, and CDKN2A (a known tumor suppressor gene that encodes the INK4A/p16 and ARF/p14 proteins)/RB1 in 72% of cases, providing evidence of common dysfunction in response to oxidative stress, squamous cell differentiation, apoptotic signaling, and/or cell cycle control, respectively. Previously unreported loss-of-function mutations were seen in the HLA-A class I major histocompatibility gene, suggesting a possible role for genotypic selection of patients for immunotherapies. Lung squamous cell carcinomas also share many alterations in common with head and neck squamous cell carcinomas without evidence of human papillomavirus infection, suggesting that the biology of these two diseases may be similar37.
Conclusion
In light of the myriad new biomarkers and targeted agents, multiplex testing strategies will be invaluable in identifying the appropriate patients for each therapy and enabling targeted agents to be channeled to the patients most likely to gain benefit. As further studies with sensitive multigene assays are completed, one might expect that the data will provide a key comprehensive means of identifying somatic alterations in entire lung cancer genomes or exomes and will ultimately inform clinical decision-making.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






