Optimal Bronchodilation for COPD Patients: Are All Long-Acting β2-Agonist/Long-Acting Muscarinic Antagonists the Same?
Article information

Abstract
Bronchodilators provide improvements in lung function and reductions in symptoms and exacerbations, and are the mainstay of pharmacological management of chronic obstructive pulmonary disease (COPD). The Global Initiative for Chronic Obstructive Lung Disease strategy recommends the use of a combination of long-acting β2-agonist/long-acting muscarinic antagonists (LABA/LAMA) as the first-line treatment option in the majority of symptomatic patients with COPD. This review provides an indirect comparison of available LABA/LAMA fixed-dose combinations (FDCs) through discussion of important efficacy and safety data from the key literature, with the objective of providing physicians with a framework for informed decision-making. LABA/LAMA FDCs provided greater benefits compared with placebo and similar or greater benefits compared with tiotropium and salmeterol/fluticasone in improving lung function, dyspnea, health-related quality of life, reducing rescue medication use and preventing exacerbations, although with some variability in efficacy between individual FDCs; further, tolerability profiles were comparable among LABA/LAMA FDCs. However, there is a disparity in the amount of evidence generated for different LABA/LAMA FDCs. Thus, this review shows that all LABA/LAMA FDCs may not be the same and that care should be taken when extrapolating individual treatment outcomes to the entire drug class. It is important that physicians consider the efficacy gradient that exists among LABA/LAMA FDCs, and factors such as inhaler devices and potential biomarkers, when choosing the optimal bronchodilator treatment for long-term management of patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disease, characterized by persistent airflow limitation and respiratory symptoms, resulting in breathlessness and poor quality of life12. In addition to significantly limiting quality of life, it has been associated with increased mortality and contributes to a significant economic and social burden on patients234. It is the fourth leading cause of death worldwide, and is projected to become the third by 203056. With increasing prevalence of smoking in developing countries, and aging populations in high-income countries, the burden of COPD is expected to increase considerably over the next 30 years178.
In Asia, the prevalence of COPD is high (6.2% as of 2012), indicating a substantial socioeconomic burden9. Exposure to smoke from biomass fuel is a risk factor for COPD in the Asia-Pacific region910; in particular, the prevalence of COPD among women exposed to biomass smoke is very high11. Differences exist between Asian and other populations in disease prevalence and clinical practices for COPD, including higher rates of COPD-associated mortality and morbidity, differences in healthcare management structure and cultural practices912.
Exacerbations are a hallmark of COPD; these acute events negatively impact health status, disease progression, and frequency of hospitalization, and contribute majorly to the total COPD burden on healthcare systems1314. The primary treatment goals of COPD are reduction in symptoms and future risk of exacerbations2. Bronchodilators provide improvements in lung function and reduce symptoms and exacerbations, and are therefore the cornerstone of pharmacological management of COPD1516. For patients with relatively few COPD symptoms and low risk of exacerbations, short-acting bronchodilators are a treatment option; these are also used as rescue medications on an “as needed” basis to improve breathlessness and exercise limitation. However, the majority of patients with significant breathlessness may require a more intensive treatment than short-acting bronchodilators alone, and long-acting bronchodilators are preferred1718. For patients uncontrolled on monotherapy, combining different classes of bronchodilators can help achieve better treatment outcomes1.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2018 does not recommend a singular long-acting β2-agonist/long-acting muscarinic antagonists (LABA/LAMA) fixed-dose combination (FDC) as the preferred choice for COPD management. Head-to-head studies among LABA/LAMA FDCs, along with previous network meta-analyses suggested that effects of all LABA/LAMA FDCs may not always be similar and that an efficacy gradient exists19202122, which potentially indicates that optimal bronchodilation with LABA/LAMA may not be a mere drug-class effect. Here, we review and compare the efficacy and safety of available inhaled LABA/LAMA FDCs for the management of COPD, with the aim of providing physicians with a framework for selection of optimal bronchodilation therapy with LABA/LAMA FDCs.
Positioning of LABA/LAMA in COPD Treatment Guidelines
GOLD 2018 recommends the use of LABA/LAMA as the first-line treatment option in the majority of symptomatic patients with COPD, and as a preferred treatment option in all patients for whom maintenance therapy is recommended1. Other guidelines such as the Spanish COPD Guidelines (GesEPOC) 2017 recommend LABA/LAMA as first-line treatment in high-risk patients, irrespective of their clinical phenotype23. High-risk COPD patients were defined as those with severe airflow limitation or high grade dyspnea or at least two moderate exacerbations or one hospital admission in the previous year, or a combination of these factors23. Moreover, a recently reported two-step treatment algorithm suggests that patients with either a modified Medical Research Council (mMRC) score >1 or with more than one exacerbation in the previous year should initiate treatment with LABA/LAMA24.
Specific to Korea, the Korean clinical practice guideline for COPD provides recommendations on diagnosis, assessment, monitoring, management, exacerbation, and comorbidities of COPD. Patients are classified into three groups based on the severity of airflow limitation, symptoms and exacerbation frequency: Ga (forced expiratory volume in 1 second [FEV1] ≥60%, mMRC 0–1 or COPD assessment test [CAT] <10, exacerbation ≤1/yr), Na (FEV1 ≥60%, mMRC ≥2 or CAT ≥10, exacerbation ≤1/yr), and Da (FEV1 <60%, exacerbation ≥2/yr or one hospitalization due to exacerbation, irrespective of symptom scores). LABA/LAMA is recommended for patients in group Na, who have severe breathlessness or show no improvement in symptoms with monotherapy or experience exacerbations. In group Da patients, LABA/LAMA can be administered as a first-line therapy along with a LAMA or ultra-LABA or LABA/inhaled corticosteroid (ICS)25.
Treatment with LABA/LAMA is recommended based on its superior results versus monocomponents and LABA/ICS, and lower risk of development of pneumonia versus ICS. A switch to ICS-containing therapy is suggested only for those patients who develop further exacerbations on LABA/LAMA therapy, and have an inflammatory profile susceptible to respond to the treatment with ICS2324.
Overview of Key Trials of LABA/LAMA FDCs
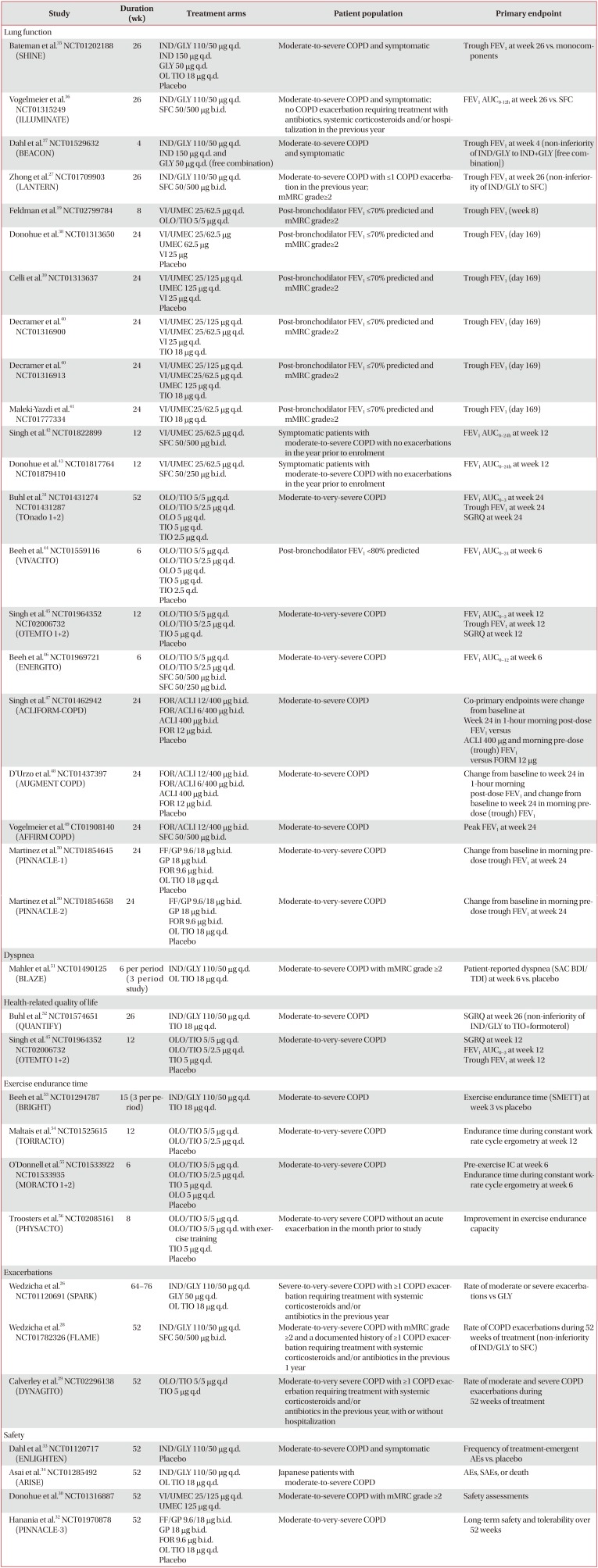
Five LABA/LAMA FDCs have been approved to date (Table 1), either as once- or twice-daily inhalations. Efficacy and safety of these LABA/LAMA FDCs have been evaluated in various placebo- and active-controlled clinical trials (Table 2)1926272829303132333435363738394041424344454647484950515253545556; active comparators mainly included the respective monocomponents, tiotropium (TIO) or salmeterol/fluticasone (SFC). Feldman et al.19 reported a head-to-head comparison of vilanterol/umeclidinium 25/62.5 µg once daily (VI/UMEC) and olodaterol/tiotropium 5/5 µg once daily (OLO/TIO) in symptomatic COPD patients. Another trial evaluating the efficacy and safety of formoterol fumarate/glycopyrrolate 9.6/18 µg twice daily (FF/GP) versus VI/UMEC 25/62.5 µg once daily is underway in patients with moderate-to-very-severe COPD (AERISTO; NCT03162055). A head-to-head study comparing the efficacy and safety of indacaterol/glycopyrrolate 27.5/15.6 µg twice daily with VI/UMEC 25/62.5 µg once daily has also been reported22.

Approved LABA/LAMA FDCs

Overview of completed Phase III studies of LABA/LAMA FDCs by the primary endpoint
Patient population, study duration and endpoints are important considerations when comparing each of these studies (Table 2). The majority of the studies included patients with moderate COPD and without exacerbation history, and evaluated change in lung function as the primary endpoint. Apart from three indacaterol/glycopyrronium (IND/GLY) studies (SPARK, LANTERN, and FLAME)262728 and one OLO/TIO trial (DYNAGITO)29, patients with recent history of COPD exacerbation were excluded from participation in the trial. The SPARK study was the first to evaluate the effect of LABA/LAMA (IND/GLY) versus LAMA (GLY and open-label TIO) on the rate of moderate or severe COPD exacerbations as a primary endpoint in patients with severe-to-very severe COPD26, followed by the FLAME study, which evaluated the annualized rate of exacerbations with IND/GLY 110/50 µg once daily versus SFC 50/500 µg twice daily (LABA/ICS) as a primary endpoint28. Recently, the 52-week DYNAGITO trial, evaluated the annualized rate of moderate-to-severe exacerbations with OLO/TIO 5/5 µg once daily versus TIO 5 µg once daily in patients with severe-to-very severe COPD29. The majority of the studies were of 24-week duration or less, with the exception of few with study duration of 52 weeks or more2628293031323334.
It should also be noted that most of these studies evaluated predominantly the Western population. A few studies/subgroup analyses have been conducted in the Asian population to address inter-ethnic differences5758596061. Furthermore, IND/GLY 110/50 µg once daily is being evaluated in mild-to-moderate COPD patients who remain symptomatic on TIO 18 µg once daily monotherapy in Korea. The primary objective of this 12-week randomized trial is to demonstrate superiority of IND/GLY over TIO in improving trough FEV157. The efficacy and safety of the U.S. approved dose of indacaterol/glycopyrrolate 27.5/15.6 µg twice daily versus monocomponents and placebo has been well established in symptomatic patients with moderate-to-severe COPD, as seen in the FLIGHT studies from the EXPEDITION trial program6263; however, this review discusses only the once-daily dosage of IND/GLY.
In terms of pragmatic/real-world evidence on LABA/LAMA effectiveness, the CRYSTAL study, a 12-week, open-label pragmatic trial, was the first to evaluate the efficacy and safety of a direct switch from previous treatments to IND/GLY 110/50 µg once daily on lung function and dyspnea in patients with moderate COPD and a history of up to one exacerbation in the previous year64. A 12-month pragmatic study comparing the time to first moderate or severe COPD exacerbation with OLO/TIO and ICS-based triple therapy is ongoing (ARWISE, NCT03265145). FLASH was a 12-week, multi-center, double-blind trial that investigated the efficacy and safety of a direct switch, without a wash-out period, from SFC 50/500 µg twice daily to IND/GLY 110/50 µg once daily in symptomatic COPD patients65. To further explore the positioning of ICS containing triple therapy in COPD management, the 26-week, double-blind, randomized, multi-center SUNSET trial has evaluated the efficacy and safety of the switch from long-term triple therapy to IND/GLY in patients with moderate-to-severe COPD with not more than one exacerbation in the previous year (NCT02603393).
Clinical Trial Evidence: Efficacy of LABA/LAMA
Efficacy of LABA/LAMA FDCs has been assessed in terms of improvement in key clinical outcomes such as lung function, dyspnea, health-related quality of life, rescue medication use, and exacerbations. These outcomes were also assessed in patients of Asian origin; results of subgroup analyses and studies in the Asian sub-populations were generally in line with those of the overall population. With very limited direct head-to-head data available, comparative efficacy of different LABA/LAMA FDCs can be evaluated only by drawing an indirect comparison between the outcomes of individual studies.
1. Lung function
Lung function outcomes for each LABA/LAMA FDC versus placebo, TIO, and SFC are presented in Table 3. In general, all FDCs improved trough FEV1 and peak FEV1. IND/GLY 110/50 µg once daily demonstrated a faster onset of action versus all comparators, while formoterol/aclidinium (FOR/ACLI) 12/400 µg twice daily and FF/GP 9.6/18 µg twice daily demonstrated it against placebo. Onset of action was reported for VI/UMEC 25/62.5 µg once daily versus placebo at 15 minutes. In the only head-to-head comparison, VI/UMEC 25/62.5 µg once daily demonstrated a significant improvement in trough FEV1 versus OLO/TIO 5/5 µg once-daily at week 8 (least square means [LSM] difference, 53 mL; 95% confidence interval [CI], 26–80 mL; p<0.0001)19. In the CRYSTAL study, IND/GLY 110/50 µg once daily significantly improved lung function after direct switch from LAMA, LABA, or LABA/ICS42. A significant improvement in lung function was also observed in patients who directly switched from SFC 50/500 µg twice daily to IND/GLY 110/50 µg once daily without a washout period in the FLASH study65.

VI/UMEC 25/62.5 µg once daily resulted in clinically meaningful and statistically significant improvements in lung function versus placebo in Asian patients with COPD58. Improvement in trough FEV1 with OLO/TIO 5/5 µg once daily versus TIO 5 µg once daily was greater in Japanese patients (change from baseline, 108 mL; p<0.0001) compared with the overall population in the TOnado trial59. IND/GLY 110/50 µg once daily demonstrated significant improvement in pre-dose FEV1 versus TIO 18 µg once daily in Japanese patients from SHINE and ARISE study61. In the Chinese cohort of the LANTERN study, IND/GLY 110/50 µg once daily showed superiority over SFC 50/500 µg twice daily, with a statistically significant and clinically meaningful improvement in trough FEV1, FEV1 area under the curve from 0 to 4 hours, and peak FEV160.
2. Dyspnea
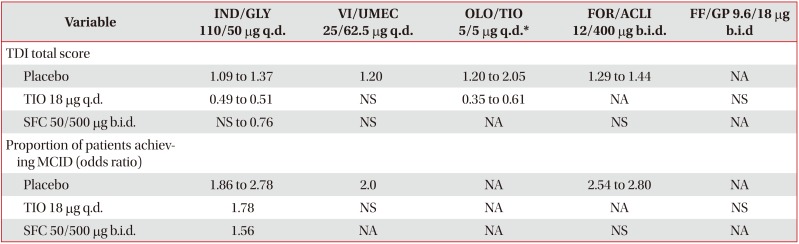
Improvement in dyspnea with LABA/LAMA FDCs was ≥1 unit on the transition dyspnea index (TDI) scale (minimal clinically important difference [MCID]) versus placebo in the majority of studies, with a greater number of patients on LABA/LAMA FDCs reaching MCID versus placebo (Table 4). IND/GLY 110/50 µg once daily significantly reduced dyspnea versus TIO 18 µg once daily and SFC 50/500 µg twice daily; OLO/TIO 5/5 µg once daily also demonstrated a significant reduction in dyspnea versus TIO 5 µg once daily. Reduction in dyspnea with other LABA/LAMA FDCs versus TIO 18 µg once daily and SFC 50/500 µg twice daily was either nonsignificant or not evaluated. In the FLASH study, patients who directly switched to IND/GLY 110/50 µg once daily from SFC 50/500 µg twice daily without a washout period showed numerical improvements in TDI total score and a greater proportion of these patients achieved MCID65.

Significant improvements in TDI total score were observed with VI/UMEC 25/62.5 µg once daily and VI/UMEC 25/125 µg once daily versus placebo (LSM treatment difference, 0.7 and 0.9, respectively) in COPD patients of Asian ancestry58. Improvement in TDI focal score was comparable between patients on IND/GLY 110/50 µg once daily and SFC 50/500 µg twice daily at week 26 (LSM treatment difference, 0.11) in the Chinese cohort of the LANTERN study38. In the Japanese cohort of the TOnado trial, OLO/TIO 5/5 µg once daily improved TDI focal score by 0.71 (p<0.05) versus TIO 5 µg once daily, which was greater than the improvement in the overall population59.
3. Health-related quality of life and rescue medication use
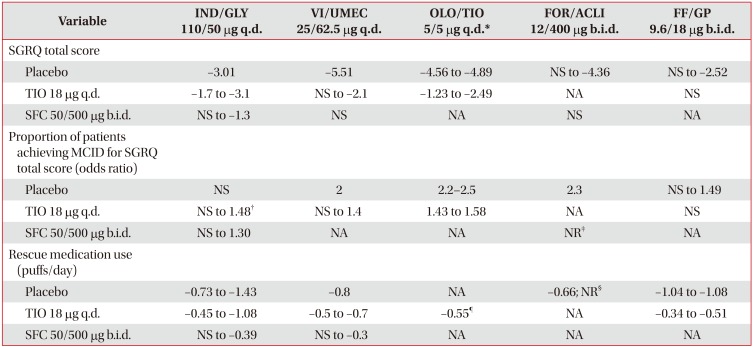
All LABA/LAMA FDCs improved St. George's Respiratory Questionnaire (SGRQ) scores and significantly increased the number of patients reaching MCID of ≥4 units versus placebo; the proportion of patients achieving MCID was not significantly greater with IND/GLY 110/50 µg once daily versus placebo (Table 5). Improvements in SGRQ total score versus SFC 50/500 µg twice daily were either non-significant or not available for LABA/LAMA FDCs, except IND/GLY 110/50 µg once daily. While improvements in SGRQ total score with IND/GLY 110/50 µg once daily were similar to those with SFC 50/500 µg twice daily in the ILLUMINATE and LANTERN studies, IND/GLY 110/50 µg once daily significantly improved SGRQ total score and the proportion of patients achieving MCID compared with SFC 50/500 µg twice daily in the FLAME study272836.

VI/UMEC 25/62.5 µg once daily and FF/GP 9.6/18 µg twice daily significantly reduced daily rescue medication use compared with TIO 18 µg once daily and placebo; furthermore, OLO/TIO 5/5 µg once daily significantly reduced rescue medication use versus TIO 5 µg once daily and FOR/ACLI 12/400 µg twice daily reduced the use versus placebo. There was a significant reduction in the use of daily rescue medication with IND/GLY 110/50 µg once daily (LSM treatment difference, −0.25; p<0.001) and VI/UMEC 25/62.5 µg once daily (LSM treatment difference, −0.3; p=0.006) versus SFC 50/500 µg twice daily2843. Daily rescue medication use was significantly less in patients receiving VI/UMEC 25/62.5 µg once daily versus OLO/TIO 5/5 µg once daily (LSM treatment difference, −0.25; p<0.001)19. The rescue medication use was comparable between IND/GLY 110/50 µg once daily and SFC 50/500 µg twice daily after 12 weeks of treatment in the FLASH study65.
Improvement in SGRQ total score was greater with OLO/TIO 5/5 µg once daily versus TIO 5 µg once daily (adjusted mean treatment difference, −3.60; p<0.05) in the Japanese subpopulation of patients from the TOnado study59. VI/UMEC 25/125 µg once daily and VI/UMEC 25/62.5 µg once daily reduced the SGRQ total score (treatment difference, −3.76 and −2.02, respectively), compared with placebo in Asian patients with COPD; the reduction was significant with VI/UMEC 25/125 µg once daily58. IND/GLY 110/50 µg once daily significantly improved SGRQ total score, compared with TIO 18 µg once daily (LSM treatment difference, −3.59; p=0.015) in the Japanese patients, with a higher proportion of patients in IND/GLY group achieving MCID61. In the Chinese cohort of the LANTERN study, a similar improvement in SGRQ total score was observed with IND/GLY 110/50 µg once daily and SFC 50/500 µg twice daily at week 26 (LSM treatment difference, −1.47; p=0.117)60.
Rescue medication use was significantly reduced with VI/UMEC 25/62.5 µg once daily (−0.6, p<0.001), while the percentage of rescue medication-free days over weeks 1–24 was greater with VI/UMEC 25/62.5 µg once daily (64.0%) compared with placebo (48.6%) in the Asian population58. In Japanese patients from SHINE and ARISE studies, IND/GLY 110/50 µg once daily significantly reduced the use of daily rescue medication versus TIO 18 µg once daily (LSM treatment difference, −0.41; p=0.013)61. Reductions in the mean daily number of puffs of rescue medication from baseline (IND/GLY 110/50 µg once daily, −1.75; SFC 50/500 µg twice daily, −1.76) and increase in the percentage of days with no rescue medication use (IND/GLY 110/50 µg once daily, 71.13%; SFC 50/500 µg twice daily, 70.16%) during the treatment period were comparable between the IND/GLY and SFC treatment groups in the Chinese cohort of the LANTERN study60.
4. COPD exacerbations
1) LABA/LAMA versus placebo or TIO
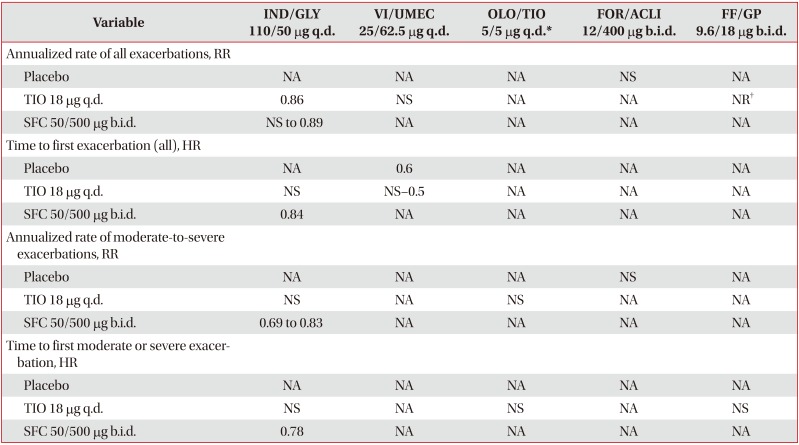
VI/UMEC 25/62.5 µg showed a decrease in the time to the first exacerbation versus placebo (Table 6). Reduction in the rate of exacerbation, though not significant, was also observed with FOR/ACLI 12/400 µg twice daily versus placebo. VI/UMEC 25/125 µg once daily reduced the risk of COPD exacerbation compared with placebo (hazard ratio [HR], 0.4; p=0.004) in Asian patients with COPD58. In patients with severe-to-very-severe airflow limitation and ≥1 exacerbation the previous year, IND/GLY 110/50 µg once daily reduced the rate of moderate or severe exacerbation by 10% versus open-label TIO 18 µg once daily (p=0.096)26. In the 52-week DYNAGITO trial, there was a numerical reduction of 7% in the rate of moderate and severe exacerbation with OLO/TIO 5/5 µg once daily versus TIO 5 µg once daily (p=0.0498); OLO/TIO 5/5 µg once daily also prolonged time to first moderate or severe exacerbation versus TIO 5 µg once daily (HR, 0.95; p=0.12); the reduction in rate and risk of exacerbation with OLO/TIO 5/5 µg once daily was non-significant29. In the 52-week PINNACLE 3 trial, 23% of patients in the FF/GP 9.6/18 µg once-daily group experienced exacerbation of any severity versus 25.1% patients in the open-label TIO 18 µg once-daily group; the time to first moderate or severe exacerbation was similar between both the groups32.

2) LABA/LAMA versus LABA/ICS
IND/GLY is the only LABA/LAMA FDC that significantly reduced the rate of COPD exacerbations compared with LAMA (GLY) and LABA/ICS (SFC) (Table 6). In the FLAME study, IND/GLY 110/50 µg once daily significantly reduced the rate of all (11%) and moderate or severe exacerbations (17%), compared with SFC 50/500 µg twice daily28. IND/GLY 110/50 µg once daily significantly prolonged the time to first exacerbation, first moderate or severe exacerbation and first severe exacerbation relative to SFC 50/500 µg twice daily, with respective risk reductions of 16%, 22%, and 19%28. In the FLASH study, the proportion of patients experiencing exacerbations was lower with IND/GLY 110/50 µg once daily versus SFC 50/500 µg twice daily65. No significant difference in the incidence of exacerbations was observed with FOR/ACLI 12/400 µg twice daily versus SFC 50/500 µg twice daily in the AFFIRM COPD trial49. COPD exacerbations (worsening), captured as safety events, occurred at a similar rate for VI/UMEC 25/62.5 µg once daily43 and OLO/TIO 5/5 µg once daily46 versus SFC 50/500 µg twice daily. In the Chinese cohort of the LANTERN study, the annualized rate of moderate or severe COPD exacerbations was significantly lower (43%) with IND/GLY 110/50 µg once daily compared with SFC 50/500 µg twice daily (rate ratio [RR], 0.57; p=0.015)60. However, with the exception of FLAME study, the remaining studies were not powered to detect an effect of treatment on exacerbation rates. No exacerbation data for FF/GP 12/400 µg twice daily versus LABA/ICS have been reported to date.
Safety of LABA/LAMA FDCs
1. Indacaterol/glycopyrronium
IND/GLY 110/50 µg once-daily demonstrated an acceptable safety profile, with adverse events (AEs) and serious AEs (SAEs) occurrence similar to placebo, TIO or SFC262728333536. In a pooled safety analysis, the hazard ratio for IND/GLY versus placebo indicated no significant increase in the overall risk for death (HR, 0.93; 95% CI, 0.34–2.54); cerebro-/cardiovascular event (HR, 0.60; 95% CI, 0.29–1.24); major adverse cardiac event (MACE) (HR, 1.04; 95% CI, 0.45–2.42); pneumonia (HR, 1.10; 95% CI, 0.54–2.25); COPD exacerbations (HR, 0.60; 95% CI, 0.40–0.91); and atrial flutter/fibrillation (HR, 1.03; 95% CI, 0.49–2.18). No significant increase in risk was observed for IND/GLY versus placebo for any of the analyzed cardiovascular (CV) safety endpoints66. The incidence of pneumonia was 3.2% in the IND/GLY group versus 4.8% in the SFC group (p=0.02) in the FLAME study28; and 0.8% versus 2.7% between these treatment groups in the LANTERN study27.
2. Vilanterol/umeclidinium
VI/UMEC 25/62.5 µg was generally well tolerated for up to 24 weeks38394041. The safety profile of VI/UMEC was generally similar to that of the placebo and comparable with that of TIO, OLO/TIO, or SFC. The most commonly reported AEs were headache (7%–10% for VI/UMEC vs. 4%–10% for all comparators) and nasopharyngitis (3%–10% for VI/UMEC vs. 2%–8% for all comparators)67. A pooled analysis of data from eight trials showed that VI/UMEC 25/62.5 µg was not associated with a clinically relevant increase in CV events. Rates of CV death, myocardial infarction, non-fatal stroke and nonfatal cardiac ischemia were ≤1% with VI/UMEC 25/62.5 µg. The trials included in this pooled analysis were not powered to detect differences in MACE outcomes68. In a head-to-head trial that evaluated VI/UMEC versus OLO/TIO, AEs were reported by 25% and 31% of patients, respectively, while 1% or fewer patients in both treatment groups reported on-treatment SAEs. No deaths were reported during the study19.
3. Olodaterol/tiotropium
The safety profile of OLO/TIO 5/5 µg was comparable with that of TIO 5 µg once daily. Treatment-emergent AEs were reported in 74.0% and 73.3% of patients receiving OLO/TIO and TIO respectively in the combined analysis of the TOnado 1 and 2 studies. Most commonly reported AE was COPD exacerbation (32.3% in OLO/TIO and 32.9% in TIO groups)31. CV SAEs and cerebrovascular SAEs occurred at a similar rate in the OLO/TIO and TIO groups, the respective rates were 1.8% and 0.5% in both the groups69. The tolerability profile of OLO/TIO in other phase III trials was generally similar to that in the TOnado trials, with no new safety concerns identified. There were no significant differences in the occurrence of AEs when comparing OLO/TIO with the monocomponents (RR, 0.99; 95% CI, 0.96–1.02) or with SFC (RR, 1.02; 95% CI, 0.85–1.23)4670. The incidence of SAEs was similar between participants receiving OLO/TIO versus monocomponents or placebo (RR, 0.99; 95% CI, 0.88–1.11)70 and versus SFC (RR, 0.80; 95% CI, 0.39–1.65)46.
4. Formoterol/aclidinium
In the ACLIFORM-COPD trial, the incidence of treatment-emergent AEs was comparable across the FOR/ACLI 12/400 µg (50.4%) and placebo (53.1%) groups; the occurrence of SAEs was low and comparable between the FOR/ACLI 12/400 µg (6.0%) and placebo (6.2%) groups47. The incidence of treatment-emergent AEs was 64.2% in the FOR/ACLI 12/400 µg group and 54.5% in the placebo group in the AUGMENT trial48. The most commonly reported AE was COPD exacerbation (9.4% in FOR/ACLI and 13.9% in placebo) in the ACLIFORM-COPD trial47 and cough (5.1% in FOR/ACLI and 3.6% in placebo) in the AUGMENT trial48. The incidence of MACE was low and comparable across both treatment arms in both studies. In the AUGMENT study, MACE based on adjudicated SAEs was reported in two patients (0.6%) in the FOR/ACLI 12/400 µg group and two patients (0.6%) in placebo group. One death was reported in the FOR/ACLI 12/400 µg group in the AUGMENT study48.
5. Formoterol fumarate/glycopyrrolate
In the 52-week PINNACLE 3 trial, the incidence of treatment-related AEs was comparable across the FF/GP 9.6/18 µg (12.5%) and TIO 18 µg (12.0%) groups; SAEs occurred in 11.0% and 10.9% of patients in the FF/GP and TIO groups, respectively. Pneumonia was reported more frequently in the FF/GP (2.5%) group, compared with the TIO group (1.3%). The incidence of MACE was low and similar across the treatment groups. Four deaths were reported in the FF/GP treatment group and five deaths were reported in the TIO group32.
Discussion
LABA/LAMA FDCs provides an effective treatment option in the management of COPD, and is recommended as the first-line treatment option in the majority of symptomatic patients with COPD. However, evidence of comparative efficacy and safety of LABA/LAMA FDCs is limited owing to scarce head-to-head comparison data among LABA/LAMA FDCs; this review tries to bridge this gap by discussing the key data on various clinical endpoints related to efficacy and safety. TIO and SFC are considered as standards of care for COPD patients, and are commonly used active comparators in LABA/LAMA trials. LABA/LAMA FDCs provided benefits greater than placebo and greater than or similar to TIO in improving lung function, dyspnea, health-related quality of life, reducing rescue medication use and preventing exacerbations. Improvements in clinical endpoints were also noted versus SFC.
While this review provides an indirect comparison between the available LABA/LAMA FDCs, some considerations should be taken into account while interpreting the results. Variability in study methodology e.g., trial duration, patient population, and endpoints, was evident. The GOLD 2018 strategy recommends the use of LABA/LAMA FDCs as an initial therapy for group D patients; however, this patient population was frequently excluded from the studies included in this review. All the studies, with the exception of the SPARK, FLAME, and DYNAGITO studies262829, did not recruit patients with very severe COPD (GOLD group D patients). Moreover, the majority of the evaluated study population excluded patients with a history of exacerbation, with the exception of three IND/GLY studies (SPARK, LANTERN, and FLAME studies)262728 and one OLO/TIO (DYNAGITO) study29. This review also discusses the evaluation of LABA/LAMA FDCs in Asian population to address the interethnic differences in treatment effectiveness. The efficacy of LABA/LAMA FDCs (IND/GLY, VI/UMEC, and OLO/TIO) in Asian population was found to be comparable with that of the overall population585960. In the Japanese cohort of the TOnado study, OLO/TIO showed greater improvements in lung function, dyspnea and health status, compared with the overall study population59. In Korea, IND/GLY is being evaluated in a 12-week trial in mild-to-moderate COPD patients symptomatic on TIO monotherapy57.
Spirometry outcomes, health-related quality of life and rescue medication use were the main endpoints studied for all the LABA/LAMA FDCs (versus placebo); data on other clinical endpoints were sparse, and not consistently reported. Improvement in lung function was consistent with all the evaluated LABA/LAMA FDCs versus placebo, LAMA and LABA/ICS. However, improvements in lung function did not always translate to similar clinical improvements in symptoms and exacerbations. While improvement in dyspnea was observed for all evaluated LABA/LAMA FDCs versus placebo except FF/GP, differences were either non-significant or not available for most of the evaluated LAMA/LAMA FDCs versus LAMA and LABA/ICS. Improvement in health status was evident for all dual bronchodilators compared with placebo and LAMA; while improvement in health status was not assessed for FOR/ACLI versus TIO, it was non-significant with FF/GP versus TIO. Furthermore, a significant reduction in the SGRQ total score was observed with IND/GLY versus SFC, with a significant proportion of patients achieving clinically meaningful improvement in the SGRQ total score; other LABA/LAMA FDCs were either not evaluated or were non-significant versus SFC in improving the health status. A significant reduction in the use of rescue medication was observed with LABA/LAMA FDCs versus placebo and TIO; data are not available for OLO/TIO versus placebo and for FOR/ACLI versus TIO.
Exacerbations were evaluated as the primary endpoint in only two trials for IND/GLY2628, and one trial for OLO/TIO29; other studies have not either evaluated exacerbations as a primary endpoint or were underpowered. FLAME was a landmark study to show superiority of IND/GLY in reducing the rate of exacerbation and improving lung function compared with SFC in exacerbating patients with moderate-to-very-severe COPD28. VI/UMEC prolonged the time-to-first exacerbation (all exacerbations) versus placebo and TIO, while IND/GLY significantly reduced the annualized rate and risk of exacerbations (all and moderate-to-severe) versus SFC. In the SPARK study, IND/GLY significantly reduced the rate of all COPD exacerbations versus TIO, while a numerical reduction was observed for the rate of moderate or severe exacerbations26. Reduction in the rate of moderate-to-severe exacerbations, though not significant, was also observed with OLO/TIO versus TIO in the DYNAGITO trial29. VI/UMEC showed no significant effects on the rate of exacerbations compared with TIO in the active comparator studies. Nevertheless, these results confirm the benefit of LABA/LAMA versus LAMA, and reinforce the role of LABA/LAMA FDCs in current treatment recommendations.
In a head-to-head study, VI/UMEC was found to be superior to OLO/TIO in improving trough FEV1; the study presented some limitations such as absence of a placebo arm, short study duration of 8 weeks and open-label administration of treatments19. In another head-to-head trial, indacaterol/glycopyrrolate 27.5/15.6 µg once daily and VI/UMEC 25/62.5 µg once daily provided clinically meaningful and comparable bronchodilation at week 1222; these results pertain to the U.S. approved dose and formulation of IND/GLY and should not be extrapolated to the formulation approved outside of the United States.
All the LABA/LAMA FDCs were found to be generally well tolerated and had similar safety profiles. No major side effects were reported with LABA/LAMA FDCs in any of the trials considered for this review. COPD worsening was the most common AE; other frequently reported AEs included cough, headache, nasopharyngitis, and upper and lower respiratory tract infections, which occurred at a similar incidence compared with placebo. Data on CV events, a common risk associated with LABAs, were inconsistent among the evaluated trials. An increased rate of pneumonia was reported with LABA/ICS, compared with LABA/LAMA2728.
Another key aspect to consider while comparing LABA/LAMA FDCs is the choice of inhaler device, which is as important as the drug molecule71, and requires careful consideration of patient's specific needs and inhaler techniques7273. The majority of the available LABA/LAMA FDCs use dry powder inhalers, while OLO/TIO is delivered using the soft-mist inhaler Respimat and FF/GP is delivered via the Aerosphere pressurized metered-dose inhaler device. Ease of use and patient satisfaction are key attributes associated with preference for a particular inhaler device747576. Patients and health care providersalso reported breath actuation as an important device attribute, as it eliminated the need for co-ordination between actuation and inspiration for effective drug inhalation74. Errors in device handling are not taken into account in clinical trials and are often underestimated in real life; on an average, more than two-thirds of patients make at least one error in device handling7778. A real-life study that evaluated handling of most frequently used inhaler devices reported that device handling errors, including critical errors, were very common in COPD patients, and were associated with severe COPD exacerbations, even for drugs and devices that were found to be effective in reducing exacerbations in controlled clinical trials79. Overall, selection of the inhaler device for LABA/LAMA FDCs is influenced by the factors described above and by evidence from both controlled and real-life assessments.
The long-term treatment of COPD with ICS has been associated with SAEs such as pneumonia8081; therefore, identification of patients who will benefit the most from ICS treatment is necessary to prevent undue exposure of patients to the above risks. In this regard, the recently concluded SUNSET trial has explored the effect of a switch from long-term ICS-containing triple therapy to IND/GLY, in non-exacerbating patients with moderate-to-severe COPD. Post-hoc analyses of several studies have evaluated blood eosinophil cut-offs that could predict the efficacy of LABA/ICS in COPD patients82838485. A recent pre-specified analysis of the FLAME study prospectively investigated the role of blood eosinophils as a predictive biomarker for the use of LABA/ICS in preventing COPD exacerbations versus a LABA/LAMA. In this analysis, IND/GLY was found to be superior to SFC in preventing exacerbations in patients with <2%, ≥2%, <3%, <5%, and <150 cells/µL blood eosinophil count. At no cut-off was SFC found to be superior to IND/GLY in preventing exacerbation86. Blood eosinophil cut-offs may predict the efficacy of LABA/ICS in preventing exacerbations versus bronchodilator monotherapy82838485, but no such evidence is available to identify patients who should receive LABA/ICS instead of LABA/LAMA FDCs. It is important to identify patients inadequately treated with ICS because this treatment should be discontinued in order to reduce the risk of side effects. Knowledge of patient's history of exacerbations and blood eosinophil counts may assist in the decision to discontinue ICS87.
Conclusion
Current evidence suggests that optimal bronchodilation with LABA/LAMA FDCs plays a vital role in COPD management including reduction of exacerbations. LABA/LAMA FDCs provide greater benefits versus placebo and active comparators in patients with COPD, although with some degree of variability. There is not an equivalent amount of evidence on efficacy outcomes for all LABA/LAMA FDCs. The large IGNITE clinical trial program has established the efficacy of IND/GLY across different outcomes in COPD patients of all severities. Additionally, the TOnado program with OLO/TIO has also provided a large amount of data about efficacy and safety of this combination in COPD. However, similar robust evidence is lacking to date for other dual bronchodilators. Therefore, care should be taken when extrapolating the findings for singular LABA/LAMA FDC to the entire drug class. Greater patient and physician education and interaction are needed to ensure the use of appropriate therapy for appropriate patients.
Notes
Authors' Contributions: Conceptualization: all authors. Methodology: all authors. Data curation: all authors. Writing - original draft preparation: all authors. Writing - review and editing: all authors. Approval of final manuscript: all authors.
Conflicts of Interest: M.M. has received speaker fees from Boehringer Ingelheim, Chiesi, Cipla, Menarini, Rovi, Grifols and Novartis, and consulting fees from Boehringer Ingelheim, Chiesi, GlaxoSmith-Kline, Gebro Pharma, CSL Behring, Novartis and Grifols. S.B., V.V., and R.L. are employees of Novartis.
The work was funded by Novartis Korea Ltd.