Diagnosis and Treatment of Latent Tuberculosis Infection
Article information
Abstract
A small number of viable tuberculosis bacilli can reside in an individual with latent tuberculosis infection (LTBI) without obvious clinical symptoms or abnormal chest radiographs. Diagnosis and treatment for LTBI are important for tuberculosis (TB) control in public and private health, especially in high-risk populations. The updated 2014 Korean guidelines for TB recommend that tuberculin skin tests, interferon-gamma release assays, or a combination of the two can be used for LTBI diagnosis according to age and immune status of the host as well as TB contact history. The regimens for LTBI treatment include isoniazid, rifampicin, or isoniazid/rifampicin. However, results of drug susceptibility test from the index case must be considered in selecting the appropriate drug for recent contacts. Standardized LTBI diagnosis and treatment based on the new 2014 guidelines will contribute to the effective TB control in Korea as well as to the establishment of updated guidelines.
Introduction
When humans are infected with Mycobacterium tuberculosis, tuberculosis (TB) only develops in 10% of those infected. TB develops in 5% of those infected, mostly within 1-2 years of M. tuberculosis infection1.
Latent tuberculosis infection (LTBI) is the state in which human are infected with M. tuberculosis without any clinical symptoms, radiological abnormality, or microbiological evidence2.
The TB burden of South Korea is intermediate, where the annual incidence of TB in 2013 was reported as 97/100,0003. LTBI treatment was not emphasized until 2011, when Korean TB guidelines included aggressive LTBI treatment. Because of frequent TB outbreaks in schools and increasing number of immune-compromised patients including the elderly, guidelines for LTBI were enhanced in 20114 and updated in 20145. In this review, we will focus on the main points and revised contents of the 2014 Korean guidelines for TB.
National Situation in Latent TB Infection
The LTBI rate in Korea, estimated by tuberculin skin test (TST) among 20-24 years old in 1985 was 74.5%, and it was 59.3%6 in 1995. The TST positive rate among 15-20 years old and young military soldiers in the mid 2000 was 20%-30%7,8; but the rate in the late 2000 and in the early 2010, in which most subjects did not receive bacillus Calmette-Guérin (BCG) revaccination, were decreased to 14%-16% in Koreans in their late teens and early twenties9.
LTBI Diagnosis Indication and Methods
1. Indication for LTBI diagnosis
LTBI diagnosis is based on the targeted TST strategy, which recommends a test for the subjects who have risk factors for developing active TB from LTBI10. In the case of suspicious new infection for subjects who had been treated for LTBI or active TB, LTBI treatment can be done considering the risk of active TB progression.
2. Diagnosis for LTBI
For LTBI diagnosis, exclusion of active TB is essential, and the old healed TB without TB treatment history among the bellowed risk groups for TB development is considered as LTBI, even without an LTBI test11. A TST test using RT-23 2TU and an interferon-gamma release assay (IGRA) test are used to diagnose LTBI. There are commercial IGRA tests such as QuantiFERON-TB Gold In Tube (QFT-IT; Qiagen, Valencia, CA, USA) and T-SPOT.TB (Oxford Immunotec, Abingdon, UK). However, these diagnostic tools do not differentiate LTBI from active TB infection.
1) LTBI diagnostic approach in immune-competent subjects
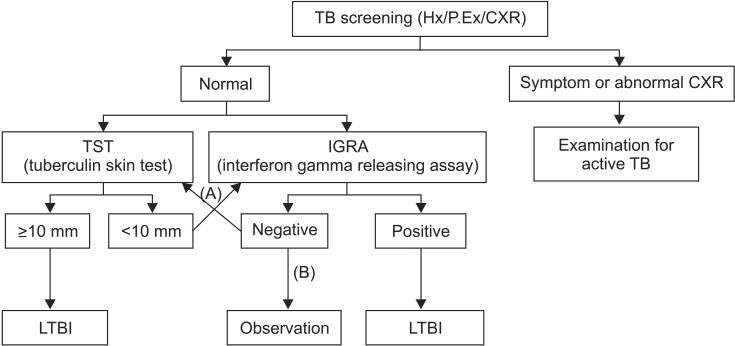
TST is the basic method to diagnose LTBI in immune-competent subjects10,12, but IGRA alone can be used13. Furthermore, a TST/IGRA two-step strategy in which the initial TST is followed by confirmatory IGRA for TST positive subjects can be used, because false positivity due to BCG vaccination or nontuberculous mycobacteria (NTM) infection can be reduced by additional IGRA test with high specificity14,15. The diagnostic approach algorithm is presented in Figure 1.

Latent tuberculosis infection (LTBI) diagnosis in immune-competent subjects. Appropriate method according to situations can be selected from the followings: TST alone (A), TST/IGRA two step test (B), or IGRA test alone (C)5. TB: tuberculosis; Hx: history; P.Ex: physical examination; CXR: chest radiographs.
2) LTBI diagnostic approach in immune-compromised subjects
IGRA alone or TST combined with IGRA can be used, but exclusion of LTBI using TST-negative result alone is not recommended. Either TST-positive or IGRA positive is regarded as LTBI in TST/IGRA combined method. The TST/IGRA two-step strategy is not recommended in immune-compromised subjects16 in contrast to immune-competent subjects17. Old spontaneously healed TB lesion without TB treatment history is regarded as LTBI, even when the LTBI test is negative. An indeterminate result on the initial IGRA test in immune-compromised subjects is frequently repeated on subsequent IGRA test18, so LTBI confirmation can be made based on TST result. The diagnostic approach algorithm is presented in Figure 2.
Latent tuberculosis infection (LTBI) diagnosis in immune-compromised subjects. Appropriate method according to situations can be tuberculin skin test (TST)/interferon-gamma release assays (IGRA) combination test (A) or IGRA test alone (B). TST-negative result alone cannot exclude LTBI, but TST-positive result alone can indicate LTBI5. TB: tuberculosis; Hx: history; P.Ex: physical examination; CXR: chest radiographs.
3. Serial TST and IGRA
1) Serial TST
A serial test refers to a TST test following an initial TST in contact investigation to exclude a false-negative result during the period of 8 weeks after the last contact with an infectious TB patient (window period); this is when the TST does not lead to complete response due to delayed hypersensitivity19. On the other hand, a two-step TST, which is usually conducted for healthcare workers, means subsequent TST 1-4 weeks after the initial TST20. This is because delayed response triggered by initial TST can appear due to recall immune phenomenon, in the subjects who are previously infected with latent TB (booster effect)19. In the subjects whose basal initial TST result is negative, TST conversion (from negative to positive) after several months can strongly suggest a new TB infection19.
Serial TST is recommended in high/moderate risk groups (Table 1) and children ≤18 years of age. In the subjects with TST <5 mm, TST conversion is confirmed with a subsequent TST ≥10 mm. In the subjects with TST 5-9 mm, TST conversion is confirmed with subsequent TST increase ≥6 mm19. This rule applies to regular follow-up checks for healthcare workers. But in contact investigation, a TST increase of ≥6 mm from the initial TST result (e.g., 3 mm to 9 mm) indicates conversion under the following conditions: highly infectious index case, close TB contacts, long duration of contact, contacts <5 years, or immune-compromised contacts19.
2) IGRA in children and adolescents
IGRA is not recommended in children <5 years of age21. An IGRA test alone is not recommended for the subjects of 5-18 years of age21,22, except under the conditions in which TST result is highly likely to be a false-positive-a BCG vaccination after 1 year or BCG revaccination22,23.
Indications for LTBI Treatment
LTBI diagnosis is based upon the premise that the subjects with a positive LTBI test must be treated. The candidates for LTBI diagnosis is categorized into two groups: those with contact with infectious TB patients and those without contact with infectious TB patients.
1. Non-contacts with infectious TB patients
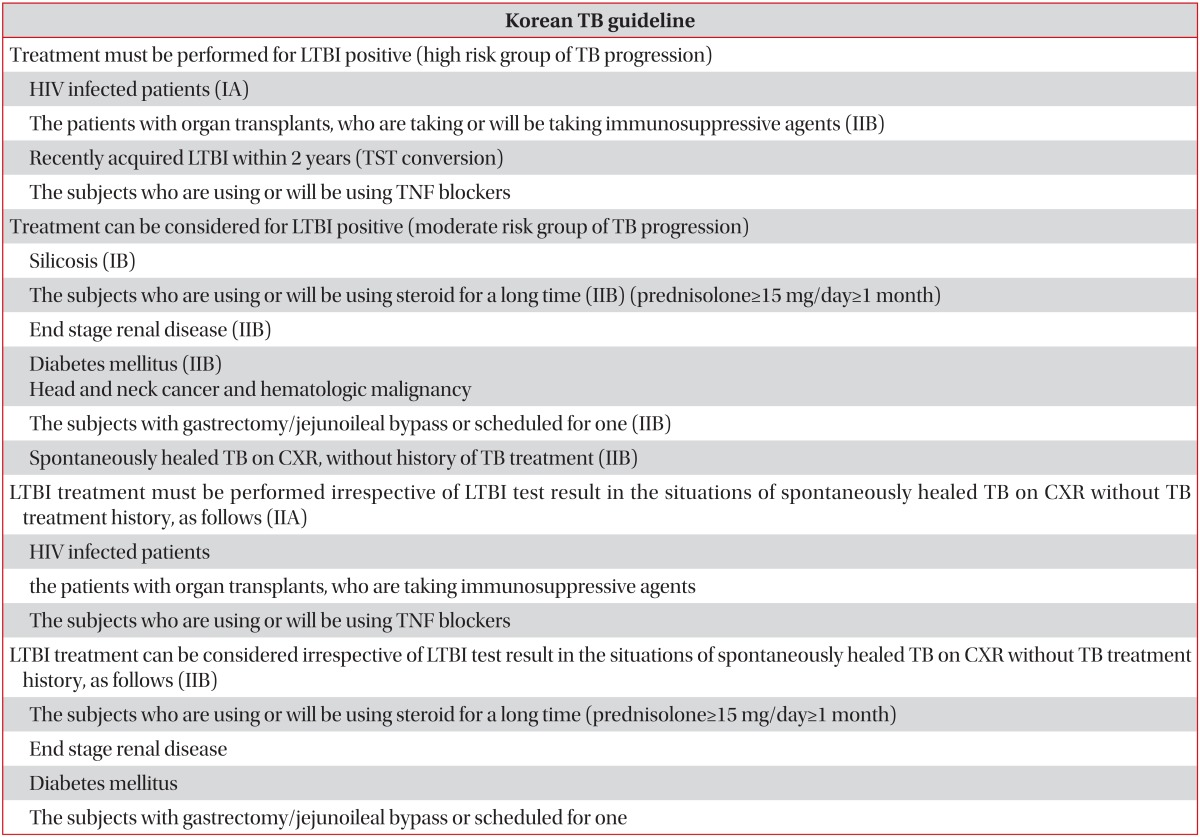
The candidates for LTBI diagnosis can be classified as high risk groups and moderate risk groups22. For the subjects with LTBI-positive in the high risk group, LTBI treatment must be conducted; but for those with LTBI-positive in the moderate risk group, LTBI treatment can be considered (Table 1). In 2014 Korean new guideline, head and neck cancer and hematologic malignancy were included in the moderate risk group24.
2. Contacts with infectious TB patients
In contact investigation condition, candidates for LTBI screening is restricted to those who are ≤35 years old, because risk owing to hepatotoxicity by anti-TB drugs exceed the benefit of LTBI treatment. For those who are ≤35 years old with LTBI-positive, LTBI treatment is obligatory17. For LTBI-positive subjects in the above mentioned high/moderate risk groups, LTBI treatment is necessary for those that had contact with an infectious TB patient (Table 2). The patients with head and neck cancer or hematologic malignancy were added for this group in the 2014 Korean guidelines.
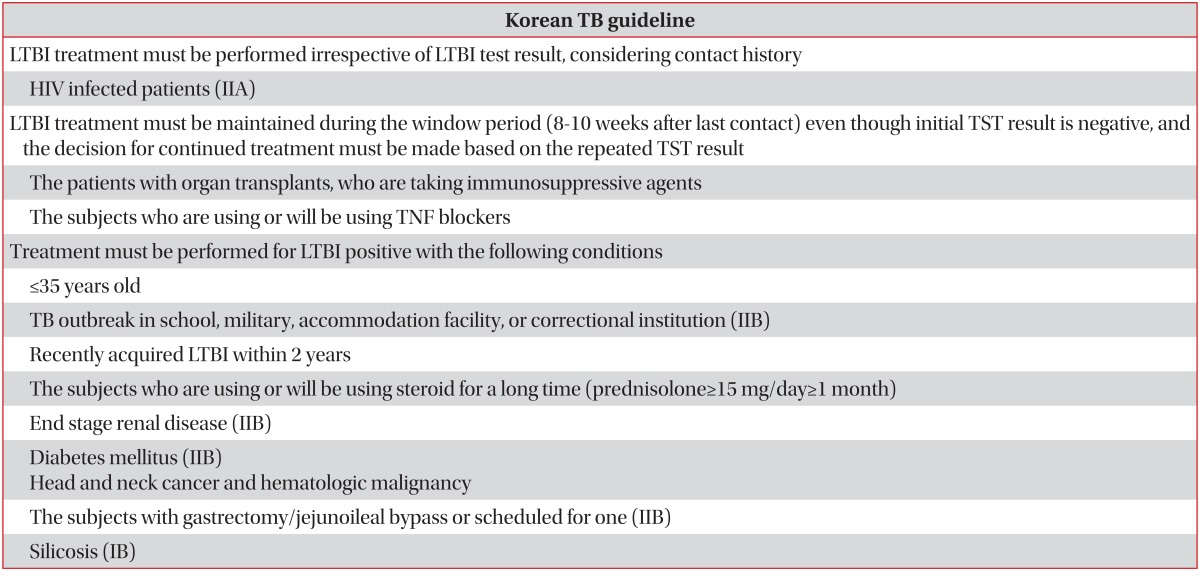
A serial repeated TST must be performed for people in the high-moderate risk group, who had an initial negative TST result after 8 weeks since their last contact with an infectious TB patients25. LTBI treatment must be maintained during the window period even though the initial TST result was negative for contacts <2 years old17, those on immunosuppressive agents who received a transplant, or those on tumor necrosis factor (TNF) α blockers.
Based on the repeated TST result after 8 weeks of window period, LTBI treatment must be continued for the contact with a positive result, but LTBI treatment can be stopped for those with a negative result. However, for the human immunodeficiency virus-positive, LTBI treatment must be continued even after a repeated TST-negative result. For the contacts with initial TST-negative result in the moderate risk group, the decision for LTBI treatment must be delayed until a repeated TST is taken after 8 weeks of window period. The risk groups are as follows: between 2-18 years of age; taking long-term steroids or scheduled to take long-term steroids; having silicosis, end stage renal failure, diabetes mellitus, head and neck cancer, or hematologic malignancy; and gastrectomy/jejunoileal bypass or scheduled for one. For contacts with TST conversion (from TST-negative to TST-positive), LTBI treatment must be performed; but for people without TST conversion (from TST-negative to TST-negative), LTBI treatment is unnecessary25.
LTBI Treatment
The drug susceptibility test (DST) from the index case must be considered when selecting the appropriated drug for recent TB contacts, and the LTBI treatments are as follows.
1. Regimens for LTBI treatment
1) Isoniazid mono treatment
Isoniazid (5 mg/kg/day, maximum 300 mg/day) for 9 months (9H) is recommended, but isoniazid for 6 months (6H) can be reasonable considering the cost-effectiveness26.
2) Short course treatment regimens containing rifampicin
(1) Rifampicin mono treatment
Rifampicin treatment for 4 months (4R) has excellent treatment completion rate, and this regimen can be given to the contacts exposed to an index case with a strain resistant to isoniazid26,27.
(2) Isoniazid/rifampicin combination regimen
Isoniazid/rifampicin combination regimen for 3 month (3HR) is recommended by the National Institutes for Health and Clinical Excellence (NICE) guideline17. This regimen has excellent treatment compliance rate28 and was reported to be superior to 9H regimen in treatment efficacy29. Moreover, isoniazid / rifapentine combination regimen (once a week for 12 weeks) was recently introduced as a new regimen30, but rifapentine is not available yet in Korea.
2. Monitoring during the LTBI treatment
Basal complete blood count, aspartate aminotransferase/alanine aminotransferase, and bilirubin must be checked before LTBI treatment. A liver function test must be checked monthly for the subjects with basal abnormal liver function test results or with risk factors. There is no method to verify complete eradication of LTBI, so TST or IGRA result does not verify complete LTBI treatment.
3. LTBI treatment in special condition
1) Pregnancy
The 9H regimen is recommended, and pyridoxine must be supplied to infant whose mother is being treated with isoniazid for LTBI. The 4R regimen can be given to pregnant women, but further investigation is needed for this regimen.
2) Contacts who contacted with the multi-drug resistant TB
Generally, LTBI treatment is not recommended due to lack of data, and follow-up for 2 years is recommended10.
4. Retreatment for LTBI
Retreatment for LTBI is considered for people in high/moderate risk groups, who had recent contact, even though they have completed LTBI treatment.
5. Treatment for active TB developed during LTBI treatment
First line standard regimen containing already prescribed drugs for LTBI treatment is recommended.
LTBI Diagnosis and Treatment in TNF Blockers Users
1. LTBI diagnosis for subjects who will use TNF blockers
The guidelines for LTBI diagnosis for these subjects is same for the guidelines for immune-compromised patients. IGRA alone or TST/IGRA combination tests can be used, but LTBI diagnosis with TST alone is not recommended. In TST/IGRA combination tests, LBTI can be confirmed by either TST-positive or IGRA-positive31. A TST-positive criterion is induration size ≥10 mm. Two-step TST can be considered, if applicable, to increase the sensitivity of LTBI diagnosis in immune-compromised subjects32.
2. LTBI treatment and active TB treatment for subjects who will use TNF blockers
Active TB detected by basal examination must be treated, and TNF blockers are recommended to be started after the completion of active TB treatment. But, TNF blockers can be started after 2 months of intensive treatment for active TB33, under the following conditions: the disease is not severe, responses to anti TB drugs are favorable, and the strain is drug-susceptible. LTBI detected by basal examination must be treated. TNF blockers are recommended to be started 3 weeks after the initial LTBI treatment34, but TNF blockers treatment and LTBI treatment may be initiated at the same time35.
3. Monitoring for TB during TNF blocker treatment
Prompt examination reacting to the symptoms suggesting TB is preferred to regular chest radiographs screening for TB development. The incidences of extrapulmonary tuberculosis, NTM disease, or severe TB are high during the uses of TNF blockers, so particular attention must be paid.
LTBI Diagnosis and Treatment in Patients with Organ Transplants
The examinations for active TB and LTBI must be performed for patients with organ transplants, who are taking or will be taking immunosuppressive agents. LTBI diagnosis comply with the guidelines for immune-compromised subjects. LTBI screening is preferably recommended before immunosuppressive agents are begun, to decrease the indeterminate result of IGRAs.
In a Korean study where TST and T-SPOT.TB tests for LTBI diagnosis and treatment were performed for 312 patients with kidney transplants, T-SPOT.TB tests for the patients with TST-negative results were useful in predicting active TB development36. Based on either TST-positive or IGRA-positive after excluding active TB, LBTI is confirmed because the concordance rate is not so high between TST and IGRAs for the patients waiting for kidney transplants37,38. In the same context, TST-positive or IGRA-positive can confirm the LTBI after excluding active TB in the subjects with organ transplants or waiting for organ transplants. The 9H regimen for LTBI treatment is recommended, but 4R or 3HR can be considered to complete the LTBI treatment before transplantation.
Conclusions
The followings are modifications in the 2014 Korean guidelines for TB, from the 2011 guidelines. Head and neck cancer and hematologic malignancy were added to the risk group for LTBI diagnosis and treatment. For non-contacts with infectious TB patients, the candidates for LTBI diagnosis and treatment were classified into a high risk group and moderate risk group. For LTBI treatment, the results of the DST from the index case must be considered in selecting the appropriate drug for recent TB contacts. The guidelines expressing IGRA's important role for the patients with organ transplants were added. In immune-compromised patients including TNF blocker users, LTBI can be diagnosed with either TST-positive or IGRA-positive, but cannot be excluded with TST-negative alone. In the public sector, LTBI screening for contacts to infectious TB patients are actively progressing with government-centered policy. In the private sector, clinicians are faced with the need to actively treat growing number of immune-compromised patients with LTBI, including the patients with organ transplants and those taking immunosuppressive agents. Conclusively, the 2014 Korean guidelines for TB, based on standardized LTBI diagnosis and treatment, is expected to be upgraded in the near future, supplementing the LTBI guidelines for growing foreign residents in an era of internationalization.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.