


What Is Extracorporeal Life Support?
Extracorporeal life support (ECLS), in particular, veno-venous (VV) extracorporeal membrane oxygenation (ECMO) is currently used as rescue therapy on patients with severe acute respiratory distress syndrome (ARDS) or severe hypoxia. Over the last five years, bridge therapy using ECLS has shown good clinical outcomes1,2.
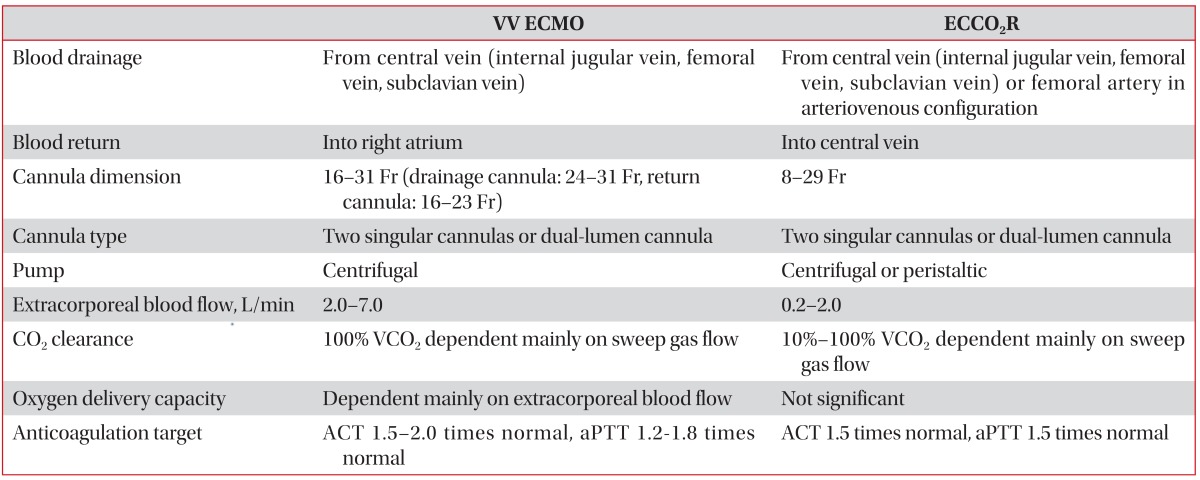
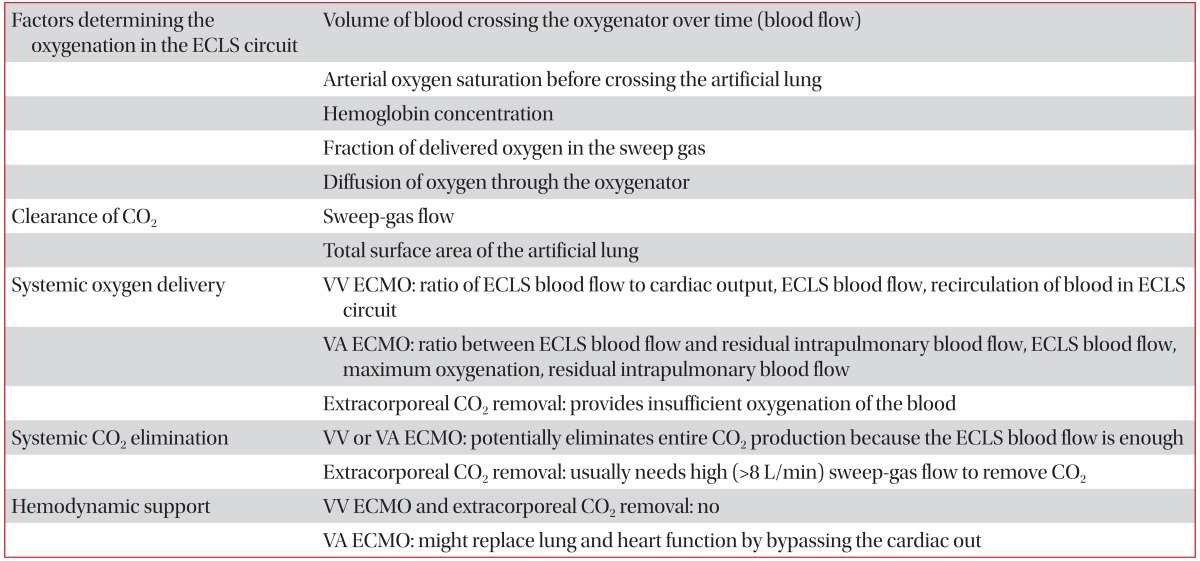
The basic principle of ECLS is that while a pump (from semi-occlusive roller-head device to centrifugal pump) drives blood flow through an oxygenator (from silicone membrane to polymethylpentene fibers) via the extracorporeal circuit, the blood interacts with constant flow of oxygen at a specific speed using sweep-gas flows (Table 1)3. Extracorporeal oxygenation and CO2 removal are determined by three factors: extracorporeal blood flow rate controlled by the centrifugal-pump speed, sweep-gas flow rate controlled by a flow meters, and oxygen tension within the sweep gas controlled by a gas blender (Table 2)3.
The ECLS strategy which is mostly applied to ARDS patients is VV ECMO, but a switch to veno-arterial ECMO can be considered if reduced cardiac function is accompanied or hypoxia progresses even during the use of VV ECMO4.
As extracorporeal CO2 removal (ECCO2R) requires low blood flow rates (1-2 L/min), small cannulas, and less anticoagulation to remove CO2, it is more convenient to deal with than ECMO5. Because of low blood flow rates, oxygen is supplied by a patient's own lungs. As another type, the pumpless arteriovenous extracorporeal circuit is also used. Here, extracorporeal blood flows are caused by the native arteriovenous pressure gradient (Ōēź60 mm Hg)6.
Considerations in Adult Patients with Respiratory Failure
There are no standardized criteria for the application of ECLS. However, it is mostly applied for rescue therapy on refractory hypoxia or hypercapnia or for ultra-protective ventilator strategies for the prevention of ventilator-induced lung injury (VILI). High ECMO flow rates (3-7 L/min) are required to improve oxygenation, and low flow rates (500-1,500 mL/min) are sufficient to remove CO2 effectively. Indication of ECLS should be decided after considering the risk-benefit ratio by multidisciplinary discussions.
1. Extracorporeal membrane oxygenation
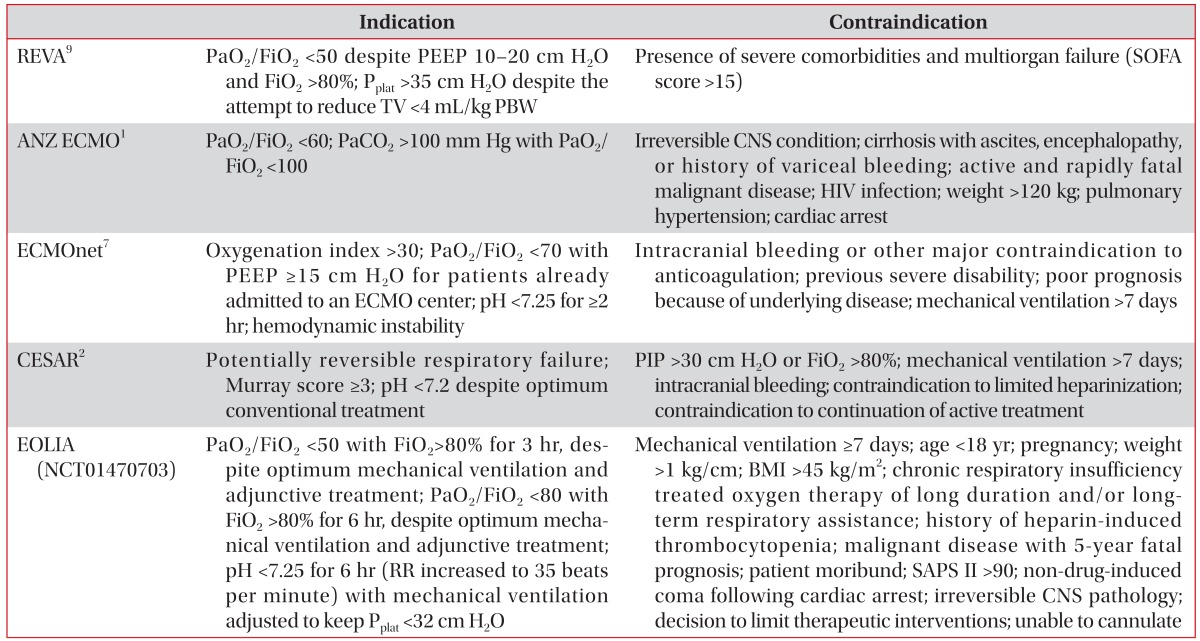
Factors deciding the application of ECLS in patients with respiratory failure are the oxygenation index, PaO2/FiO2, Murray score, and refractory hypercapnia with acidosis (Table 3).
In 2009 H1N1 influenza epidemic, many centers applied ECMO to patients with severe ARDS and refractory hypoxia. Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECOMO) Influenza Investigators1 reported a survival rate of 75% in the ECMO treatment group. The Italian ECMO Network also showed a survival rate of 68% in the ECMO treatment group7. The Swine Flu Triage (SWiFT) study, done in the UK showed the lower in-hospital mortality in the ECMO treatment group (24% vs. 53%, p=0.006)8. In the CESAR trial, severe ARDS patients also showed the higher survival rate in the ECMO treatment group (63% vs. 47%, p=0.03)2.
The above results suggested that the implementation of protective mechanical ventilation during ECMO can improve the prognosis.
EOLIA (NCT01470703) should help to define the clinical efficacy of VV ECMO in severe ARDS patients.
2. Extracorporeal CO2 removal
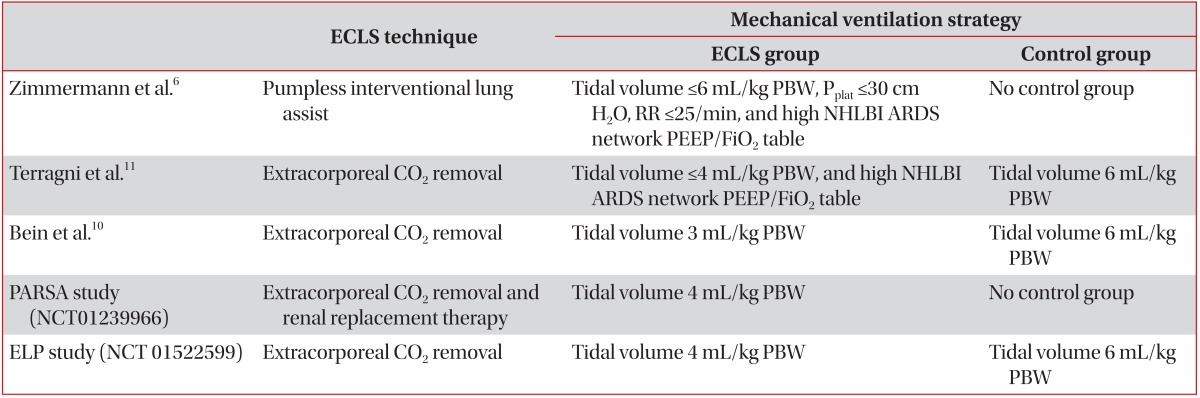
Recent studies reported that the application of ECCO2R in ARDS patients can reduce the lung injury as it enables the ultraprotective strategies of mechanical ventilation (Table 4). Zimmermann et al.6 reported that when pumpless AV ECLS was applied to 51 patients with ARDS, low tidal volume ventilation could be maintained along with the continuous removal of CO2, and the survival rate was 50%.
A randomized, controlled study was done to compare an ultra-protective mechanical ventilation (3 mL/kg predicted body weight [PBW] with Pumpless AV ECLS) with low tidal volume ventilation (6 mL/kg PBW) strategies in 79 patients with ARDS. While the two groups did not differ for in-hospital mortality, within the patient group with PF ratio <200, the ultra-protective group showed an improved survival10. At present, studies on the efficacy of very low tidal volumes ventilation strategies during ECCO2R are working in progress.
Controversies
1. Mechanical ventilation strategies
For minimizing VILI, the ventilator settings during VV ECMO should be maintained at low levels to enable the prevention of atelectasis while keeping the alveoli open. However, there are no specific recommendations other than the maintenance of positive end-expiratory pressure (PEEP) at 10 cm H2O or above. As the injured lungs contribute little to oxygenation, lung recruitment using PEEP while maintaining minimal tidal volumes might accelerate lung healing or optimise cardiopulmonary function12,13.
In the CESAR trial, lung rest was induced by limitation of the peak inspiratory pressure to 20 cm H2O with PEEP 10 cm H2O, 10 breaths per minute, and FiO2 of 30%. Another study also showed positive outcomes in patients who maintained a mean plateau pressure of 25 cm H2O9.
2. Tracheostomy
In the case of applying ECLS due to severe ARDS, mechanical ventilation for a long period of time is predicted. Therefore, the early tracheostomy might be considered. The use of anticoagulants during ECLS is not the contraindication for tracheostomy. In a recent study, a tracheostomy with the percutaneous dilatational technique done by experienced physician is safe with a brief interruption of anticoagulation. In this study, no major complications such as death were observed16.
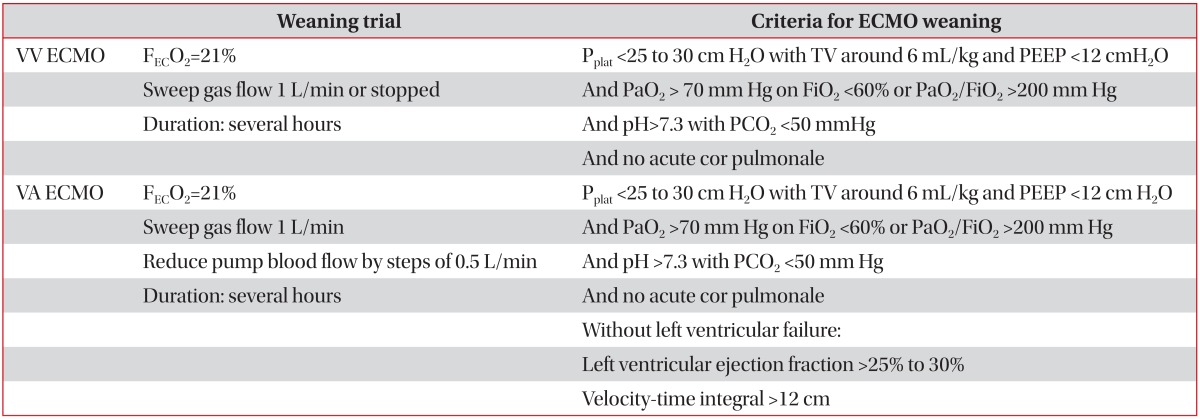
3. Weaning from ECLS (Table 5)17
When mechanical ventilation settings is acceptable (tidal volume <6 mL/Kg PBW, plateau pressure <30 cm H2O, PEEP <12 cm H2O, FiO2 <60%) and respiratory mechanics, gas exchanges, and radiographic findings are improved, weaning from ECLS can be considered. Before weaning, the existence of acute cor pulmonale should be identified. Two main strategies of weaning can be used: reducing sweep-gas flow rates or reducing extracorporeal blood-flow rates. Alternatively, weaning of mechanical ventilation may be considered earlier than weaning from ECLS18,19.
4. Sedation
While deep sedation and neuromuscular blockade might be required in the initial stages to relieve symptoms and reduce oxygen consumption, patients should be kept awake to actively participate in rehabilitation therapy during ECLS. In addition, early mobilization could suppress the progression of weakness and reduce the incidence of delirium.
The indication for the use of awake ECMO, instead of invasive mechanical ventilation is not confirmed in patients with ARDS refractory to non-invasive ventilation. However, the use of awake ECMO as a bridge before lung transplantation has shown promising results20,21,22,23. Mechanical ventilation and sedation might worsen outcomes before and after the transplantation. Awake ECMO enables patients to communicate, eat, and walk and improves physical and physiological conditions.
5. Technological advances
The first technological advances in this field may be the production of bicaval dual-lumen cannulas24. This cannula is inserted via the right internal jugular vein, and then drains blood from the superior and inferior vena cava through one lumen and returns blood into the right atrium through a second lumen. Only one cannulation enables patients to receive intensive physiotherapy more conveniently. Second, reduction in the size of ECLS equipment has enabled patients receiving ECLS to transfer and mobilise25.
6. Anticoagulantion and transfusion
Although the ECLS circuits are engineered with biocompatible materials, the systemic anticoagulants are still required to prevent thrombotic complication. Unfractionated heparin is most commonly used and monitoring is performed using activated partial thromboplastin time (1.2-1.5 times control), anti-Xa activity (0.2-0.4 IU/mL), or the activated clotting time. When heparin-induced thrombocytopenia is suspected, argatroban or bivalirudin can be used as alternatives26.
The guidelines of the Extracorporeal Life Support Organization (ELSO) recommend maintaining normal hemoglobin concentration for tissue oxygenation. However, some centers is more restrictive to transfusion thresholds in critically ill patients (Hb <7 g/dL).
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






