


Introduction
IgG4-related disease is newly recognized fibroinflammatory condition characterized by edema of invaded organ, a dense lymphoplasmacytic infiltration rich in IgG4-positive plasma cells, storiform pattern of fibrosis, and, often but not always, elevated serum IgG4 concentration level1,2. The most commonly involved organs are pancreas and salivary gland. It may also intrude thyroid, retroperitoneum, kidney, lung, and lymph node, but the invasion of lung is rare1,2,3. IgG4-related lung disease may be asymptomatic or has symptoms such as cough, hemoptysis, dyspnea, and chest pain1,2,3. IgG4-related lung disease could appear as solitary nodular lesion, thickening of bronchovascular bundles, interlobular septa, roundshaped ground-glass opacity (GGO), honeycombing, and bronchiectasis in chest computed tomography (CT), and it is difficult to discern that it comes from other lung diseases4.
In this paper, we report a case that a patient who came to hospital due to hemoptysis and had lung mass in chest CT was diagnosed IgG4-related disease by biopsy.
Case Report
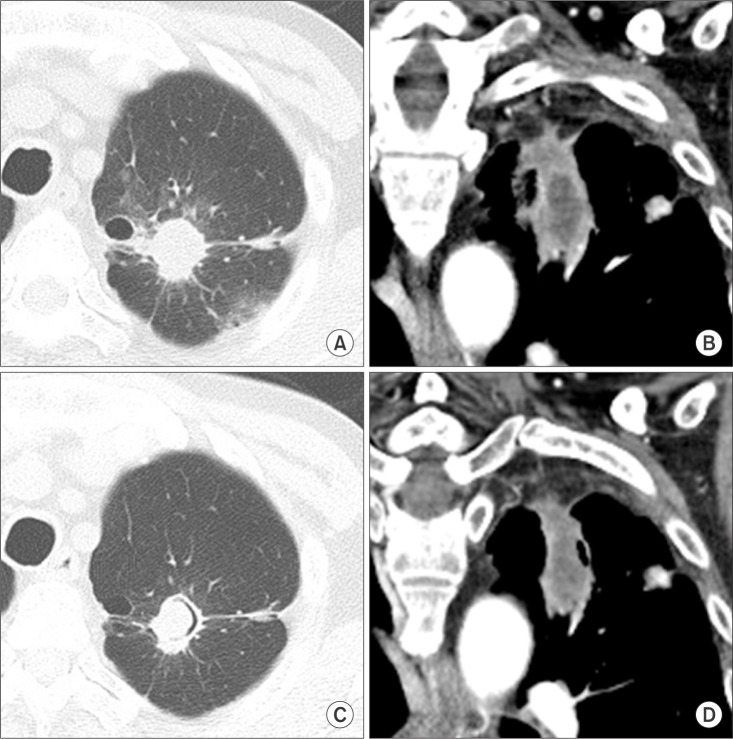
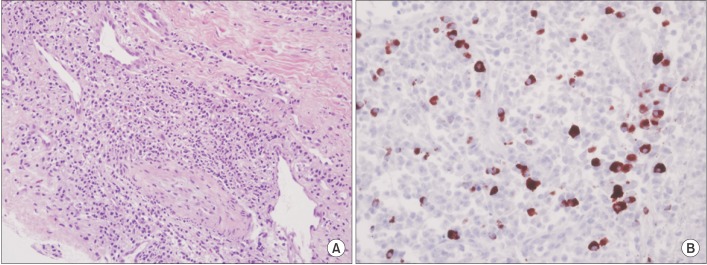
A 63-year-old man visited the pulmonary clinic complaining hemoptysis which has lasted for 5 days. His past medical history were pulmonary tuberculosis (completely healed 20 years ago), diabetes mellitus, hypertension, and chronic kidney disease. He did not smoke and drink. There was no specific family history. Lung sound was clear and heart sound was normal without murmur. There was no palpable mass or lymph node in the neck. Blood pressure was 130/70 mm Hg, body temperature was 36.8Ōäā, pulse rate was 92 beats per minute, and respiratory rate was 20 breaths per minute. Laboratory findings revealed hemoglobin 8.4 g/dL, white blood cell 4,530/mm3 (neutrophils, 64.3%; lymphocytes, 21.7%; eosinophils, 4.5%), platelets 234,000/mm3, C-reactive protein 1.10 mg/dL, aspartate aminotransferase 16 IU/L, alanine aminotransferase 9 IU/L, total bilirubin 0.26 IU/L, creatinine 2.72 mg/dL, blood urea nitrogen 33 mg/dL, and hemoglobin A1c 10.4%. In chest X-ray a simple mass was noted at left upper lobe, which was not found in the past film. In chest CT about 4.1-cm irregular shaped mass with spiculated margin was seen at left upper lobe (Figure 1A, B). We performed bronchoscopy and transthoracic needle biopsy. In bronchoscopy, there were no specific endobronchial findings and bronchial washing smear for acid-fast bacilli was negative. Transthoracic needle biopsy showed multiple scattered infiltrations of IgG4-positive plasma cells more than 40 in high-power field (Figure 2B), lymphoplasmacytic infiltration and a storiform pattern of fibrosis (Figure 2A). Although serum IgG (1,010 mg/dL; normal range, 670-1,600 mg/dL) and IgG4 (25.1 mg/dL; normal range, 6.1-121.4 mg/dL) levels were not elevated because the biopsy showed typical IgG4-related disease pathologic finding, we diagnosed as IgG4-related lung disease. There were no specific findings of pancreas in abdomen CT. After the patient was treated with oral glucocorticoids, hemoptysis disappeared and the size of mass was decreased (Figure 1C, D).
Discussion
Since IgG4-related pancreatitis was reported by Hamano et al. in 2001 for the first time5, IgG4-related disease has been identified in other organs such as salivary gland, gallbladder, thyroid, retroperitoneum, and kidney. The first case of IgG4-related lung disease in Korea was reported by Yoo et al. in 20096, and a few cases have been reported ever since. According to the presentation of Inoue et al. in 20094, IgG4-related lung disease could be categorized into four major subtypes: solid nodular type having a solitary nodular lesion that includes a mass; round-shaped GGO type characterized by multiple round-shaped GGOs; alveolar interstitial type showing honeycombing, bronchiectasis, and diffuse GGO; and bronchovascular type showing thickening of bronchovascular bundles and interlobular septa. In Korea, total nine cases of IgG4-related lung disease have been reported. These cases showed multiple lung nodules or mass6,7, consolidative mass8, pleural nodules or mass9,10, pleural effusion11, interstitial lung disease12, or bronchovascular bundle thickening13 in chest CT, and accompanying symptoms were cough, sputum, fever, dyspnea, or asymptomatic. All serum IgG4 levels in Korea cases elevated except the case of bronchial thickening with eosinophilic angiocentric fibrosis patient, in which case serum IgG level was normal and serum IgG4 level was not mentioned 6,7,8,9,10,11,12,13. However, in our case presenting symptom was hemoptysis and serum IgG4 level was normal.
Solitary pulmonary lesion could be malignancy, infectious granuloma (e.g., aspergillosis and tuberculosis), harmatoma, or nonspecific granuloma14. Lesion larger than 3 cm was called mass and is often malignant14. Therefore, we performed biopsy.
The critical histopathologic features of IgG4-related disease are a dense lymphoplasmacytic infiltration, a storiform pattern of fibrosis, and obliterative phlebitis15. Furthermore, the diagnosis of IgG4-related disease rests on both presence of the characteristic histopathological appearance and increased numbers of IgG4-positive plasma cells infiltration. Elevated serum concentrations of IgG4 are found in approximately 70% of patients with IgG4-related disease1. In this case even though serum IgG4 level was normal, histopathologic feature of lung biopsy showed dense lymphoplasmacytic infiltration, storiform pattern of fibrosis (Figure 2A), and more than 40 IgG4-positive plasma cells in high-power field (Figure 2B). Thus, we diagnosed as IgG4-related lung disease.
Although the optimal treatment for IgG4-related disease has not been established yet, it has been known that glucocorticoids have an effect on most IgG4-related disease patients. The effects of glucocorticoids are alleviation of symptoms, reductions of mass size, improvement of organ function, and decrease in serum levels of IgG41. In this case patient was treated with methylprednisolone 0.4 mg/kg for 1 month and methylprednisolone was tapered. After 1 month of treatment, hemoptysis disappeared and lung mass size was decreased as well (Figure 1C, D).
This case showed that solitary lung mass with normal serum IgG4 level could be IgG4-related lung disease and IgG4-related lung disease could present hemoptysis.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






