Treatment of Isoniazid-Resistant Pulmonary Tuberculosis
Article information

Abstract
Tuberculosis (TB) remains a threat to public health and is the leading cause of death globally. Isoniazid (INH) is an important first-line agent for the treatment of TB considering its early bactericidal activity. Resistance to INH is now the most common type of resistance. Resistance to INH reduces the probability of treatment success and increases the risk of acquiring resistance to other first-line drugs such as rifampicin (RIF), thereby increasing the risk of multidrug-resistant-TB. Studies in the 1970s and 1980s showed high success rates for INH-resistant TB cases receiving regimens comprised of first-line drugs. However, recent data have indicated that INH-resistant TB patients treated with only first-line drugs have poor outcomes. Fortunately, based on recent systematic meta-analyses, the World Health Organization published consolidated guidelines on drug-resistant TB in 2019. Their key recommendations are treatment with RIF-ethambutol (EMB)-pyrazinamide (PZA)-levofloxacin (LFX) for 6 months and no addition of injectable agents to the treatment regimen. The guidelines also emphasize the importance of excluding resistance to RIF before starting RIF-EMB-PZA-LFX regimen. Additionally, when the diagnosis of INH-resistant TB is confirmed long after starting the first-line TB treatment, the clinician must decide whether to start a 6-month course of RIF-EMB-PZA-LFX based on the patient's condition. However, these recommendations are based on observational studies, not randomized controlled trials, and are thus conditional and based on low certainty of the effect estimates. Therefore, further work is needed to optimize the treatment of INH-resistant TB.
Introduction
Despite the availability of anti-tuberculosis (TB) chemotherapy, TB remains a threat to public health and is the leading global cause of death by a single infectious agent. Approximately 10 million people worldwide develop TB annually, and 1.6 million die from the disease1. In South Korea, about 30,000 new cases of TB occur and around 2,000 people die from TB23. TB is a highly infectious disease in which about 30% of closely contacted people become infected and about 5%–15% of infected people develop TB throughout their lifetimes456.
Isoniazid (INH) is an important first-line anti-TB agent because of its potent early bactericidal activity. However, resistance to INH, alone or in combination with other drugs, is now the most common type of resistance to anti-TB drugs. Global data on INH resistance without concurrent rifampicin (RIF) resistance were 7.1% in new TB cases and 7.9% in previously treated TB cases1. Unfortunately, the global burden of INH-resistant TB is not decreasing. A representative United States study published in 2008 reported that the prevalence of INH-resistant TB had not declined, despite the downward trend in the prevalence of overall TB7. Data from the World Health Organization (WHO) showed that resistance to INH was detected in 30% of TB cases in Eastern Europe and 14% of TB cases in West/Central Europe and Africa from 1994 to 20098. National surveys and cohort studies in South Korea showed that the prevalence of INH-resistant TB over the past 20 years was approximately 10% in new cases and >30% in previously treated cases91011121314.
The management of INH-resistant TB is important because of its unsatisfactory outcomes compared to drug-susceptible TB1516. Previous systematic meta-analyses have shown that resistance to INH reduces the probability of treatment success and increases the risk of acquiring resistance to other important first-line drugs such as RIF, thereby increasing the risk of multidrug-resistant (MDR)-TB1718. Moreover, INH-resistant TB generally requires longer treatment than drug-susceptible TB, increasing the burden of the disease.
Guidance on the management of INH-resistant TB is under debate, in contrast to the consensus for the management of patients with drug-susceptible or MDR-TB. Studies performed in the 1970s and 1980s showed low rates of treatment failure for patients with INH-resistant TB receiving four or five first-line drugs in 6-month regimens1920. However, recent data have shown that patients with INH-resistant TB who received only first-line regimens have worse outcomes than those with drug-susceptible TB16182122. Several previous international guidelines have recommended the addition of a fluoroquinolone (FQ) to strengthen anti-TB treatment regimens for INH-resistant TB, particularly for cases of extensive disease23242526. However, little research has supported this recommendation, and no definitive randomized or controlled study has been performed. Thus, current treatment regimens for INH-resistant TB vary2728293031323334, and the optimum regimen including use of an FQ or duration of treatment had remained controversial35. In 2019, based on comprehensive systematic meta-analyses on the management of INH-resistant TB2236, the WHO published consolidated guidelines on drug-resistant TB, including INH-resistant TB37. Here we review studies and international guidelines on the management of INH-resistant TB.
Isoniazid Resistance
After the introduction of INH for treatment of TB in the 1950s, resistance to INH emerged38. Generally, “INH-resistant” TB refers to strain with resistance to INH and susceptibility to RIF confirmed in vitro, regardless of concurrent resistance to other anti-TB drugs. “INH mono-resistance” TB refer to resistance to a single first-line drug such as INH, and susceptibility to any other anti-TB drugs39. Resistance to INH is usually due to a mutation in katG or inhA, and is less commonly due to mutations in other genes, such as the ahpC32 gene4041. INH is a prodrug that must be activated by catalase-peroxidase, an enzyme regulated by katG, to be effective against TB. Mutations in katG, most commonly at Ser315Thr, can result in high-level resistance to INH4243. The inhA gene encodes an enoyl acyl carrier protein reductase involved in fatty acid synthesis in M. tuberculosis. Because these fatty acids are the targeted by the active derivative of INH, mutations in inhA or its promoter region block INH binding and result in low-level INH resistance44. Isolates with an inhA mutation are also typically resistant to ethionamide and prothionamide45.
In Mycobacterium tuberculosis, drug resistance develops through spontaneous genetic mutations. Thus, the development of acquired drug resistance usually occurs when there is a large bacterial population, such as in pulmonary cavities46 or when an inadequate drug combination or dosage is prescribed1547. Rarely, malabsorption of anti-TB drugs may account for acquired resistance48. Risk factors for developing INH resistance have been reported, and most studies have found a strong correlation between a history of TB treatment and INH resistance. In an analysis of drug-resistant TB trends in the United States, a history of TB, foreign birth, and Asian or Pacific Islander ethnicity were found to be risk factors for INH resistance2949. Similarly, in Germany and Israel, a history of TB treatment was identified as a risk factor for INH resistance5051.
Burden of Isoniazid Resistant TB in South Korea
The prevalence of drug-resistant TB is used as a surrogate marker for the performance of national tuberculosis control programs. INH resistance could serve as an indicator of drug resistance to TB because INH is inevitably used in the initial treatment regimens. From the 1960s to the 1990s, nationwide TB prevalence surveys were conducted in South Korea, and initial and acquired resistance to anti-TB drugs in patients with culture-confirmed TB were enumerated (Table 1)91011. In the surveys, the prevalence of INH resistance was found to have increased significantly from 25% in 1965 to 44% in 1980, and decreased markedly thereafter to 22% in 19909. From the 1990s to 2004, a further four surveys of TB patients registered for treatment at health centers were conducted in South Korea (Table 1)12. During the survey period, the prevalence of drug-resistant TB decreased markedly due to improved treatment efficacy. However, since 1994, the incidence of INH resistance has increased in new cases and decreased in retreatment cases.

The rates of resistance to anti-TB drugs in six university hospitals in South Korea in 2010 have been reported13. Among 542 M. tuberculosis isolates from patients with pulmonary TB, including 473 (87%) from new cases and 69 (13%) from previously treated cases, the rates of INH resistance were approximately 14%. Recently, a study was conducted to evaluate the drug-resistance rates of 5,599 clinical M. tuberculosis isolates collected from 2010 to 2014 at seven tertiary hospitals in South Korea14. In that study, 4,927 (88%) were from new cases and 672 (12%) were from previously treated cases, with INH resistance rates of 11% and 35%, respectively. Therefore, the burden of INH-resistant TB in South Korea is still considerable.
Previous Studies on the Treatment Outcomes of Isoniazid-Resistant TB
1. Ineffectiveness of first-line drug regimens for isoniazid-resistant tuberculosis
No definitive randomized or controlled studies have been performed to date that have determined the optimal treatment regimen for patients with INH-resistant TB. Thus, in this chapter, we describe key studies on the management of INH-resistant TB. A number of clinical trials conducted by the British Medical Research Council in the 1970s and 1980s showed that patients with INH-resistant TB responded well to 6-month chemotherapy regimens that included RIF and pyrazinamide (PZA) with treatment success rates above 95%19. Based on these data, in 1994 the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC) recommended a 6-month treatment regimen for INH-resistant TB52. Patients with INH-resistant TB were recommended to receive RIF, ethambutol (EMB), and PZA for 6 months. Several subsequent international guidelines also recommended combination regimens of first-line anti-TB drugs for INH-resistant TB535455, supported by the results of several studies27295657585960.
However, since the late 1990s to early 2000s, several studies yielded results that conflicted with those of the above studies (Table 2). The use of only first-line anti-TB drugs for INH-resistant TB occasionally resulted in poor outcomes. Moreover, the acquisition of additional drug resistance upon treatment failure was a concern. In a controlled trial in 1997 in India comparing three short-course regimens of first-line anti-TB drugs, an unfavorable response and relapse occurred in 17%–62% and 8%–25% of 227 patients with INH-resistant TB, respectively61. Notably, among 74 patients with INH-resistant TB who had an unfavorable response, 23 (31%) had acquired resistance to RIF. In 2000, the outcomes of standard short-course therapy for drug-resistant TB in Dominica, Hong Kong, Italy, Russia, South Korea, and Peru were published16. Of 457 INH-resistant TB patients, 82 (18%) had unfavorable outcomes, including failure (2%), death (4%), default (6%), and transfer (6%), suggesting that INH resistance is associated with unfavorable outcomes of treatment with first-line regimens16. In a 2004 Russian retrospective study that included 180 patients with INH-resistant TB, but not MDR-TB, who received the WHO standardized short-course or retreatment regimen, the unfavorable outcome rate was 30%, comprised of 17 (9%) deaths, 21 (12%) treatment failures, 11 defaults (6%), and five transfer (3%)62. Similarly, in a large study in Georgia including 889 INH resistant TB patients treated for 9 months with RIF-EMB-PZA, 135 (15%) had unfavorable treatment outcomes21. In addition, studies in Israel51, Taiwan63, Mexico64, and India65 reported unfavorable outcome rates of 7%–44% among patients with INH-resistant TB treated with first-line drugs. Therefore, patients with INH-resistant TB could have worse outcomes, even when treated with a first-line regimen or the WHO-retreatment regimen. These findings are probably because previous studies may not adequately reflect the clinical characteristics in a real-world population of patients with many underlying diseases. These data suggest the need for a more effective regimen for patients with INH-resistant TB.

Treatment outcomes of patients with isoniazid-resistant tuberculosis in previous studies
2. Acquisition of resistance to additional drugs
Acquisition of additional drug resistance, especially for RIF, is an important concern during the treatment of INH-resistant TB using first-line regimens, and can lead to the emergence of MDR-TB. Studies on the acquisition of drug resistance have steadily been reported, especially among patients who had unfavorable outcomes after treatment of INH-resistant TB. For example, in a report from South Korea, a patient with INH-resistant TB acquired MDR during 12 months of treatment with RIF-EMB, with PZA administered during the initial 2 months66. The authors subsequently reported the outcomes of 39 patients with INH-resistant TB who were treated with first-line anti-TB drug regimens28. Treatment failure occurred in three (8%), and MDR was identified in two of the three patients during treatment for 2 months with INH-RIF-EMB-PZA and 10 months of RIF-EMB treatment. In an Indian study of 1,817 patients with TB, although resistance to RIF emerged in only 2% of the patients, 32 of 60 patients (53%) with INH-resistant TB who had unfavorable outcomes acquired resistance to RIF67. A 2011 South African study evaluated the outcomes of a retrospective cohort of 155 patients with INH-resistant TB who received the standard first-line four-drug therapy for 1 year68. In that study, 14 of 23 patients (61%) whose therapy failed progressed to MDR-TB, although the retreatment cases also received streptomycin (SM) for the first 2.5–3.5 months.
3. Use of FQs for isoniazid-resistant TB
Former WHO and United States guidelines recommended the addition of an FQ to strengthen anti-TB regimens for INH-resistant TB, especially for patients with extensive disease23242526. Although little clinical evidence initially supported this recommendation, recent studies have verified the benefit of addition of an FQ30697071. In a Danish study in 2002–2007, 40 of 110 patients (36%) with INH-resistant TB were additionally treated with an FQ, resulting in treatment success in 36 (90%)30. In a retrospective study in South Korea of 140 patients with INH-resistant TB, treatment failure was more frequent among the patients who did not receive FQs than those who did (6/65, 9% vs. 1/75, 1%; p=0.049)69.
Similarly, in a Taiwanese study of 395 patients with INH-resistant TB, supplementation with an FQ significantly improved the treatment success rate (60% vs. 13%, p=0.003)70. In a retrospective study in Canada, 12 of 165 patients (7%) with INH-resistant TB had an unfavorable outcome of treatment with first-line drugs with or without addition of a FQ32. Interestingly, no relapse occurred in the 61 patients (37%) who received an FQ-containing regimen. Additionally, in a large retrospective study in Peru, the treatment outcomes of 947 patients with INH-resistant TB who were treated with a standardized 9-month regimen of RIF-EMB-PZA plus levofloxacin (LFX) were evaluated72. In that study, death and treatment failure occurred in only 18 (2%) and 12 cases (1%), respectively, although 186 cases (20%) were lost to follow-up. These data suggest that the addition of an FQ may enhance the treatment of INH-resistant TB.
4. Systematic reviews and meta-analyses of isoniazid-resistant TB
Several recent meta-analyses of INH-resistant TB have indicated the limited efficacy of regimens consisting of only first-line anti-TB agents against INH-resistant TB. In 2009, Menzies et al.18 analyzed whether standardized first-line drugs or WHO retreatment regimens are appropriate for patients with INH-resistant TB or retreatment cases. Interestingly, among the six cohort studies included in that meta-analysis, the treatment failure rates were 18%–44% for INH-resistant TB. Thus, given that the WHO regimen was designed for resource-poor settings with a low initial prevalence of drug resistance, standardized empirical treatment without drug susceptibility testing could be contributing to MDR, particularly when there is a high prevalence of INH resistance.
Gegia et al.22 performed a meta-analysis that included 3,744 patients with INH-resistant TB and 19,012 with INH-susceptible TB from nine cohort studies and 33 trials. Treatment of INH-resistant TB with the WHO standardized regimen for new patients (2 months of INH-RIF-EMB-PZA followed by 4 months of INH-RIF) resulted in treatment failure, relapse, and MDR in 11%, 10%, and 8%, respectively, of the patients. While the rates for patients with drug-susceptible TB who received the standard retreatment regimen were 1%, 5%, and 0.3%, respectively. More importantly, among the patients with initial INH-resistant TB who acquired drug resistance, 96% (205/214) acquired MDR. Finally, overall failure, relapse, and acquired drug resistance were more common in patients with INH-resistant TB than those with drug-susceptible TB treated with standardized regimens of first-line drugs.
In 2018, Fregonese et al.36 evaluated the optimal duration and combination of anti-TB drugs for INH-resistant TB among 3,923 patients with INH-resistant TB from 23 cohort studies. Compared with a daily regimen of 6 months of RIF-EMB-PZA, extending the duration to 8–9 months had similar outcomes. Another notable finding was that the addition of an FQ to 6 months or more of RIF-EMB-PZA was associated with a significantly greater treatment success rate (adjusted odds ratio [aOR], 2.8; 95% confidence interval [CI], 1.1–7.3), but had no statistically significant impact on mortality or the acquisition of RIF resistance. Also, the use of an FQ plus 1–3 months of PZA (6 months of RIF-EMB and 1–3 months of PZA plus FQ) was more likely to be associated with treatment success than a 6-month RIF-EMB-PZA regimen. However, the small number of patients limited the statistical power. Interestingly, addition of SM during the initial months of treatment was associated with worse outcomes in patients with INH-resistant TB.
International Guidelines for the Management of Isoniazid Resistant TB
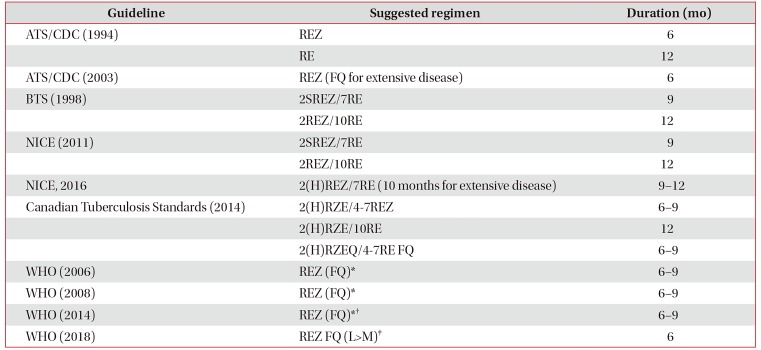
The recommended regimens for INH-resistant TB differ among countries and have differed over time. In this chapter, we summarize previous and current international guidelines for the treatment of INH-resistant TB (Table 3).

International guidelines for isoniazid-resistance tuberculosis treatment
1. United States
The ATS and CDC published guidelines in 199452. These guidelines stated that INH should be discontinued upon diagnosis of INH-resistant TB. Additionally, these guidelines recommended (1) 6 months of daily RIF-EMB-PZA if PZA was included in the initial regimen or (2) 12 months of daily RIF-EMB if PZA was not included. Subsequently, revised guidelines published in 2003 recommended 6 months of RIF-EMB-PZA for INH-resistant TB and added that an FQ may enhance the regimen for patients with extensive disease23.
2. United Kingdom
In 1998 the British Thoracic Society recommended a regimen for INH-resistant TB53. If INH resistance had been identified before starting treatment, a regimen of 2 months of SM-RIF-EMB-PZA followed by 7 months of RIF-EMB was recommended. However, if INH resistance was identified after treatment initiation, they recommended that INH treatment be discontinued and replaced by 12 months of RIF-EMB treatment.
The 2011, National Institute for Health and Care Excellence (NICE) guidelines recommended the same regimen as the 1998 British Thoracic Society guideline54. However, in the 2016 revised NICE guidelines, 2 months of RIF-EMB-PZA (±INH) followed by 7 months of RIF-EMB was recommended. In cases of extensive disease, the continuation phase could be extended to 10 months55.
3. Canadian Tuberculosis Standards
The 2014 Canadian Tuberculosis Standards recommended that patients suspected of having INH-resistant TB should be treated with all four first-line drugs while the result of drug susceptibility testing is pending73. INH could be discontinued upon identification of INH resistance, but INH could be continued if the level of resistance is low. Notably, the guidelines stated that an FQ would be equally efficacious74 and an FQ is interchangeable with INH for the treatment of INH-resistant TB. Thus, the guidelines recommended three regimens: (1) 2 months of daily RIF-EMB-PZA (±INH) followed by 4–7 months of daily RIF-EMB- PZA20 or (2) followed by 10 months of daily RIF-EMB, or (3) 2 months of daily RIF-EMB-PZA-FQ (±INH) followed by 4–7 months of daily RIF-EMB-FQ.
4. Previous WHO guidelines for the management of isoniazid-resistant TB
The 2006 and 2008 WHO guidelines stated that if INH mono-resistance is known or suspected at the time of treatment initiation, the addition of EMB to INH, RIF, and PZA in the intensive phase is recommended; and RIF-EMB-PZA can be administered for 6–9 months in the continuation phase. The guidelines also stated that for patients with more extensive disease, the addition of an FQ and prolongation of treatment to a minimum of 9 months can be considered2526.
The 2014 WHO guidelines recommended the same regimens for INH-resistant TB24. However, the 2014 WHO guidelines emphasized the need for monitoring acquisition of resistance to RIF when the RIF-EMB-PZA regimen is used to treat mono-INH-resistant TB. Because susceptibility testing to EMB and PZA is not considered reliable, infection with an INH mono-resistant strain, and not a poly-resistant strain, can be unclear at the start of treatment24. Thus, the guidelines recommended that patients not responding clinically and remaining smear- or culture-positive after 2–3 months should be tested using the Xpert MTB/RIF assay to determine RIF resistance; an MDR-TB regimen should be adopted if RIF resistance is detected. Thus, the WHO recommended use of the Xpert MTB/RIF at months 0, 2, and 3.
5. New WHO guidelines for isoniazid-resistant TB
Based on the most recent meta-analyses on the management of INH-resistant TB182236, the WHO in 2018 issued evidence-based policy recommendations for the treatment of patients with INH-resistant TB39. In 2019, the WHO formally published “consolidated guidelines on drug-resistant TB treatment”37. The key recommendations for treatment of INH-resistant and RIF-susceptible TB are (1) treatment with RIF-EMB-PZA-LFX for 6 months and (2) no addition of SM or other injectable agents to the treatment regimen.
The most notable aspect of these guidelines is that an FQ, preferably LFX, should be included in the treatment regimen for INH-resistant TB. The new guidelines, which are based primarily on individual patient data or observational studies conducted in various settings3236, indicate that supplementation with an FQ may enhance the efficacy of treatment regimens for INH-resistant TB. The evidence review of the guidelines emphasized that the treatment success rate was higher when an FQ was added to RIF-EMB-PZA regimens compared to ≥6 months of RIF-EMB-PZA (aOR, 2.8; 95% CI, 1.1–7.3). The addition of an FQ to a 6-month RIF-EMB-PZA regimen tended to reduce the number of deaths (aOR, 0.4; 95% CI, 0.2–1.1) and the acquisition of RIF resistance (aOR, 0.10; 95% CI, 0.01–1.2).
Regarding selection of an FQ, interestingly, the new WHO guidelines recommend LFX as the first choice rather than moxifloxacin. This is because LFX has a better safety profile than other FQs and was frequently used in the studies reviewed. Also, LFX has fewer drug interactions than moxifloxacin; in particular, LFX is less affected by RIF. For example, the plasma peak concentration of LFX is not affected by the addition of RIF7576. Additionally, there are no contraindications for the use of LFX with antiretroviral agents, which is important for patients infected with human immunodeficiency virus. However, LFX has contraindications: (1) cases in which resistance to RIF cannot be excluded, (2) known or suspected resistance to LFX, (3) known intolerance to FQ, (4) known or suspected risk for a prolonged QTc interval, and (5) pregnancy or breastfeeding (not an absolute contraindication). Thus, if an FQ cannot be used, patients with INH-resistant TB may be treated with RIF-EMB-PZA for 6 months.
The duration of treatment for INH-resistant TB is specified as not more than 6 months in the new WHO guidelines. Regarding the total treatment duration, a previous meta-analysis demonstrated that a 6 month RIF-EMB-PZA regimen had a higher likelihood of treatment success than a regimen of >6 months36. However, there is a risk of hepatotoxicity with the newly recommended regimen for INH-resistant TB due to the long-term use of PZA and RIF simultaneously. Drug-induced hepatotoxicity is not uncommon with anti-TB drugs, particularly with the prolonged use of PZA, which was demonstrated in patients on RIF and PZA for latent TB infection77. Thus, the patients in whom PZA treatment can be maintained for long periods are difficult to identify. A previous meta-analysis showed that, when PZA is discontinued due to adverse effects, a reduction in the duration of treatment with PZA to less than 3 months can result in worse outcomes, even with the addition of SM36. However, the optimum duration of treatment with PZA is unclear.
In the new WHO guidelines, the addition of SM or other injectable agents to the treatment regimen is not recommended. This is primarily based on a recent meta-analysis that showed that the addition of SM (≤3 months) to a RIF-EMB-PZA regimen with <4 months of PZA treatment decreased the likelihood of treatment success36, although an effect that may in part be due to confounding. Additionally, the addition of SM did not reduce the mortality rate significantly. Also, there was no clear evidence that the addition of INH benefits or harms patients. Although the data on the use of high-dose INH were insufficient, in vitro evidence suggests that in the presence of inhA mutations but not katG mutations, increasing the dose of INH is likely to be effective. However, in the presence of katG mutations, which typically confer higher-level resistance, the use of even high-dose INH is less likely to be effective78.
Therefore, in clinical practice, several points should be considered when treating INH-resistant TB. First, before starting the RIF-EMB-PZA-LFX regimen, resistance to RIF must be excluded by genotypic or phenotypic methods. Preferably, resistance to FQ, and if possible to PZA, should be excluded prior to treatment to prevent the acquisition of resistance to other drugs. Empirical treatment of INH-resistant TB is generally not advised, but in cases in which INH-resistant TB is strongly suspected (e.g., close contacts of patients with active TB but without laboratory confirmation of INH resistance), the RIF-EMB-PZA-LFX regimen may be introduced pending laboratory confirmation of INH resistance if RIF resistance has been reliably excluded.
Second, in patients in whom INH-resistant TB is confirmed after treatment with the standardized regimen (2 months of INH-RIF-EMB-PZA followed by 4 months of INH-RIF), the RIF-EMB-PZA component drugs should be continued and LFX should be added when RIF resistance has been excluded. The duration of a RIF-EMB-PZA LFX regimen is usually determined by the need for 6 months of LFX treatment. Thus, in cases in which INH-resistant TB is diagnosed after initiation of first-line TB treatment, the patient may undergo at least 6 months of drugs by the end of treatment. When INH resistance is confirmed late during the standardized regimen, the clinician must decide, based on the patient's condition, whether a 6-month course of RIF-EMB-PZA-LFX should be started at that point.
Conclusion
INH is an important first-line agent for the treatment of TB due to its potent early bactericidal activity. Resistance to INH is now the most common type of TB resistance. Studies in the 1970s and 1980s found a low rate of treatment failure for INH-resistant TB cases receiving 6-month regimens comprising four or five first-line drugs; however, recent studies have shown that INH-resistant TB patients treated with only first-line drugs have poor outcomes. Based on recent comprehensive systematic meta-analyses, the WHO published new consolidated guidelines on drug-resistant TB in 2019. Their key recommendations are (1) treatment with RIF-EMB-PZA-LFX for 6 months and (2) no addition of SM or other injectable agents to the treatment regimen. Thus, the guidance emphasizes the importance of excluding resistance to RIF before starting RIF-EMB-PZA-LFX treatment of INH-resistant TB. Additionally, when the diagnosis of INH-resistant TB is confirmed, long after starting first-line TB treatment, the clinician must decide whether to start a 6 month course of RIF-EMB-PZA-LFX, based on the patient's condition. However, these recommendations are based on observational studies, not randomized controlled trials, and are thus conditional and based on low certainty in the estimates of effect. Therefore, further work is needed to optimize the treatment of INH-resistant TB.
Notes
Authors' Contributions:
Conceptualization: Jhun BW, Koh WJ.
Writing - original draft preparation: Jhun BW, Koh WJ.
Approval of final manuscript: all authors.
Conflicts of Interest: Dr. Won-Jung Koh served on Advisory Boards for Johnson and Johnson and Insmed, not associated with the submitted work. Dr. Byung Woo Jhun has no conflicts of interest.
Funding: No funding to declare.