Recent Trends in the Prevalence of Chronic Obstructive Pulmonary Disease in Korea
Article information
Abstract
Chronic obstructive pulmonary disease (COPD) had been considered the only major disease that is continuing to increase in prevalence. There were a few studies about the change of the prevalence of COPD, which showed the prevalence of COPD did not increase. In this review, we report on the trends in the prevalence of COPD in Korea using the data from Korea National Health and Nutrition Examination Survey (KNHANES). The prevalence of COPD in 2015 was 13.4% (male, 21.6%; female, 5.8%). The prevalence of COPD did not change much, which ranged from 13.1% to 14.6% during the period from 2010 to 2015. Among the subjects found to have COPD by spirometry, only 2.8% had been diagnosed as COPD by physicians during the period from 2011 and 2015. In conclusion, the prevalence of COPD did not change significantly during the period from 2010 to 2015. And most COPD patients still had not been diagnosed by physicians and consequently had not been treated appropriately.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent and progressive airflow limitation1. COPD has emerged as a serious public health concern in recent years, and is predicted to become the fourth leading cause of death worldwide by 203012.
The worldwide prevalence of COPD has been estimated to be 7.5%–10%3. In a nationwide COPD prevalence survey in Korea in conjunction with the second Korea National Health and Nutrition Examination Survey (KNHANES II) conducted 2001, 17.2% of Korean adults over the age of 45 years had COPD4. And, follow-up studies reported in 2011 showed the prevalence of COPD was 13.4% and 12.9%56.
There were a few studies about the change of the prevalence of COPD, which showed the prevalence of COPD did not increase78.
In this article, we briefly review the trends in the prevalence of COPD in Korea from 2007 to 2015 using the data from KNHANES9.
Korea National Health and Nutrition Examination Survey (KNHANES)
KNHANES is an ongoing surveillance system in the Republic of Korea that assesses the health and nutritional status of Koreans, monitors trends in health risk factors and the prevalence of major chronic diseases, and provides data for the development and evaluation of health policies and programs in Korea. KNHANES was initiated in 1998 by the union of “National Nutrition Survey” and the “National Health and Health Behavior Survey.” Since then, surveys for the KNHANES I, II, III, IV, V, and VI have been executed. The first three KNHANES were conducted as a triannual survey. To reduce the limitation of seasonal variations, beginning with the fourth KNHANES in 2007, it was converted to an annual survey to provide timely national statistics. The survey for the KNHANES VII is under progress since 2016. The KNHANES uses rolling sampling survey method for the sample in each year to present the whole nation and to be similar by years. Twenty households were selected throughout 192 regions each year and 10,000 individuals aged 1 year and over were targeted for KNHANES9.
In KNHANES, spirometry was performed by four technicians, each of whom underwent education sessions on pulmonary function test (PFT) and quality control56. Spirometry was performed using dry rolling seal spirometers (Model 2130; SensorMedics, Yorba Linda, CA, USA) and the American Thoracic Society/European Respiratory Society criteria for the standardization of PFT10. The prediction equation used in KNHANES was derived from the KNHANES II11. The results of spirometry in each enumeration districts were stored on web-hard to investigate whether the results satisfied acceptability and reproducibility criteria of spirometry for quality control and quality assurance. For analysis on results of spirometry, only results showing two or more acceptable curves and meeting reproducibility criteria were used6.
Also, trained interviewers administered the questionnaire at the time of spirometry, to determine whether (1) the subject had a history of COPD, such as chronic bronchitis or emphysema; (2) had been diagnosed with COPD by a physician; and (3) had been treated for COPD9.
The participants aged over 40 years recording less than 0.7 of forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) were defined to have COPD56. To explore the trends of COPD prevalence from 2007 to 2015, KNHANES used age-standardized prevalence which was calculated using the age- and sex-specific structures of estimated population based on the 2005 Korea Census9.
Prevalence and Awareness of COPD
1. Prevalence of COPD in 2015
In 2015, the prevalence of COPD was 13.4% (male, 21.6%; female, 5.8%) (Table 1). This figure was similar to those of previous studies56. The prevalence of the elderly aged over 65 years recorded 28.1% (male, 45.5%; female, 13.7%). And the prevalence became higher at older age by recording 4.1%, 9.7%, 21.2%, and 30.6% in the participants in their 40s, 50s, 60s, and 70s, respectively (Figure 1). In addition, the prevalence of COPD was higher in low income subjects than that of high income subjects (Table 1).

Prevalence of chronic obstructive pulmonary disease in 2015, stratified by age and income
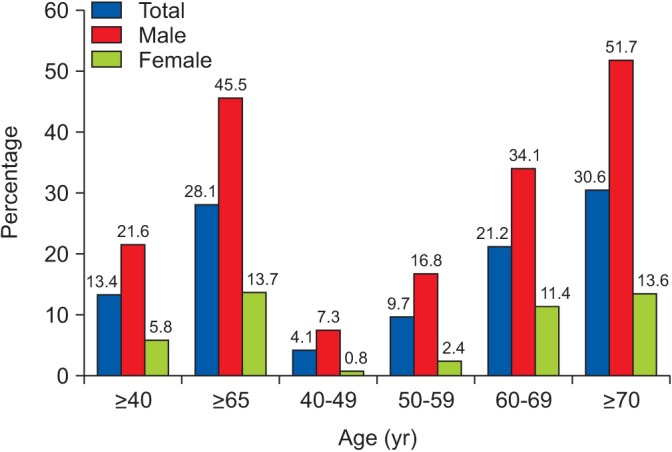
Prevalence of chronic obstructive pulmonary disease in 2015, stratified by age and gender.
2. Trends in prevalence of COPD
After conversion of annual survey during KNHNES IV, the prevalence of COPD seemed to be decreasing. However, the prevalence of COPD did not change much after 2010, which ranged from 13.1% to 14.6% during the period from 2010 to 2015 (Table 2).

Prevalence of COPD during the period from 2007 to 2015 (%)
KNHANES used the age- and sex-specific structures estimated population based on the 2005 Korea Census to explore the trends in prevalence of COPD. The age-standardized prevalence of COPD showed similar pattern (Table 2, Figure 2). This non-increase tendency of prevalence was comparable to other studies78.

Trends in age-standardized prevalence of chronic obstructive pulmonary disease.
3. Awareness of COPD
It is well known that the public awareness of COPD is limited121314 and a significant number of COPD patients have undiagnosed1516. Among the subjects found to have COPD by spirometry, only 2.8% had been diagnosed as COPD by physicians during the period from 2011 and 2015. The treatment rate was 1.6% (Table 3). This figure did not improve compared to previous studies56.

Awareness of chronic obstructive pulmonary disease (%)
4. Limitations of KNHANES
KNHANES had some limitations. First, it did not exclude other diseases associated with airflow obstruction such as bronchiectasis and tuberculous destroyed lung because it did not utilize chest radiography. Second, the existence of airflow obstruction was evaluated with a fixed ratio using FEV1/FVC <0.7, so that the prevalence of the elderly could be overestimated. Moreover, as the golden standard of detecting COPD was based on postbronchodilator spirometry, KNHANES used only prebronchodilator test.
Conclusion
The prevalence of COPD among Korean adults aged over 40 years was 13.4% in 2015. The prevalence of COPD did not change significantly during the period from 2010 to 2015. And most COPD patients still had not been diagnosed by physicians and consequently had not been treated appropriately.
Acknowledgments
We appreciate all the efforts of the Korea National Health and Nutrition Examination Survey of Korea Centers for Disease Control and Prevention (KCDC).
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.


