


Introduction
Chronic obstructive pulmonary disease (COPD) is a complex and heterogeneous disease, characterized by chronic inflammation in the airways by noxious particle such as tobacco smoking1. Secondary systemic inflammation from airway is a key feature of COPD pathogenesis2,3. Elevation of white blood cells (WBC) count, C-reactive protein (CRP), interleukin 6 (IL-6) and 8 (IL-8), and fibrinogen values in the peripheral blood have been reported in COPD patients3,4,5,6,7,8. However, systemic inflammation is also observed in other diseases such as metabolic syndrome9,10,11,12,13 and may be a consequence of these frequently accompanying comorbidities. The aim of our study was to determine whether plasma WBC count can be used as a biomarker reflecting disease severity independent of these comorbidities in COPD patients. Since current guideline assess COPD severity by pulmonary function testing and symptoms score, relationship between WBC count, lung function, and quality of life was compared by using data from Korean National Health and Nutrition Examination Survey (KNHANES).
Materials and Methods
1. Study design and participants
The KNHANES is a collection of nationally representative, cross-sectional, population-based health and nutritional surveys by the Korean Centers for Disease Control and Prevention since 1998. The participants were chosen by proportional allocation system sampling with multistage stratification, based on the geographical area, age, and sex. KNHANES includes a health interview, physical examination, laboratory tests, and nutritional questionnaires. Pulmonary function tests (PFTs) were performed for subjects >40 years of age, and among them, COPD patients were selected according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guideline1. All individuals participated voluntarily and provided written informed consent. The KNHANES protocol was approved by the Institutional Review Board of the Korean Centers for Disease Control and Prevention.
2. Measurement of variables
The PFTs were performed for subjects aged >40 years according to guidelines of the American Thoracic Society/European Respiratory Society14 using a spirometry system (model 1022; SensorMedics, Yorba Linda, CA, USA). Spirometry was repeated at least three times to ensure reproducibility and validity, and calculated based on the predictive equation for the Korean population15. The current GOLD guideline classifies COPD patients not only by the degree of airflow limitation, but also by various symptom scores, such as the modified Medical Research Council dyspnea scale or COPD assessment test (CAT) score1. KNHANES included EuroQoL which is 5-item self-administered, scale-based, generic questionnaire (EQ-5D) for quality of life (QoL) measurement in various chronic diseases such as COPD16. Since good correlations between the EQ5D and St. George's Respiratory Questionnaire (SGRQ) scores17,18, and the SGRQ and CAT scores19 have already been reported, the symptom scores were replaced by the EQ-5D in this study. The EQ5D comprises a descriptive system and a visual analog scale (VAS). The descriptive assessment includes five items: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each item can be used to represent profiles of health status or can be converted to a summary index (EQ5D-index). The VAS is a measurement scale ranging from 0 (worst health status) to 100 (best health status).
3. Definitions
COPD was defined as a pulmonary function test result of forced expiratory volume in 1 second (FEV1, L)/forced vital capacity (FVC, L) <0.7 among adult >40 years of age according to the GOLD guidelines. The degree of airflow limitation was classified as GOLD 1 if FEV1 >80%, GOLD 2 if FEV1 >50% to ≤80%, GOLD 3 if FEV1 >30% to ≤50%, and GOLD 4 if FEV1 ≤30%1. Body mass index (BMI) was calculated as kg/m2. Hypertension was defined as blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, or subjects who were already taking anti-hypertensive medication. Diabetes was defined as a fasting glucose level of ≥126 mg/dL or hemoglobin A1c of ≥6.5%, and/or diabetes treatment. Dyslipidemia was defined as an abnormal high-density lipoprotein level (<40 mg/dL in males and <50 mg/dL in females), a triglyceride level of >150 mg/dL, and/or hyperlipidemia treatment. The definition of central obesity followed the criteria for Asian individuals (waist circumference ≥90 cm for males and ≥80 cm for females)20.
4. Statistical analysis
KNHANES was designed using a complex, stratified, multistage probability-sampling model; thus, data were analyzed via the complex-sample design using stratification, sampling weight variables, and clustering variables to represent Korean population using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). In order to compare the characteristics of each subgroup, Student's t tests or analyses of variance were used to compare continuous variables and chi-square tests were used to compare categorical variables. Associations between variables were examined using Pearson's correlation coefficient (r). To determine the association between lung function and WBC count in COPD patients, general linear regression was conducted with age, sex, height, BMI, current smoking status, hypertension, diabetes, and dyslipidemia as co-variables. With respect to the association between QoL and WBC count, adjustment were made for age, sex, BMI, current smoking status, COPD severity, hypertension, diabetes, and dyslipidemia for multivariable analysis. A p-value of <0.05 was used to indicate statistical significance.
Results
1. Characteristics of the participants
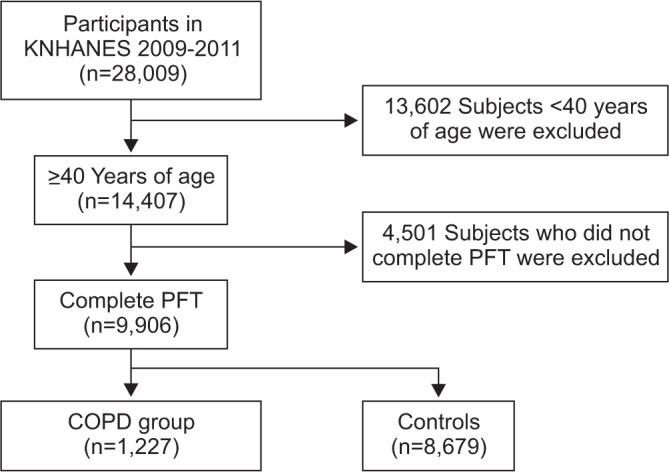
Data from a total of 9,906 adults >40 years of age were retrieved from KNHANES. Among them, 1,227 patients met the definition of COPD (Figure 1). The prevalence of COPD was 12.4%, and among them, 44.8% were classified as GOLD 1, 50.2% as GOLD 2, 4.5% as GOLD 3, and 0.5% as GOLD 4. The demographic and clinical characteristics of the COPD and non-COPD groups are summarized in Table 1. Between the non-COPD and COPD groups, age, sex, height, BMI, and smoking status were significantly different, and the prevalence of hypertension, diabetes, and dyslipidemia was much higher in the COPD group; the values of cholesterol, WBC count, hemoglobin, platelet count, blood urea nitrogen, creatinine, QoL (both EQ5D-index and EQ5D-VAS), and pulmonary function were different between the groups.
2. WBC count and lung function
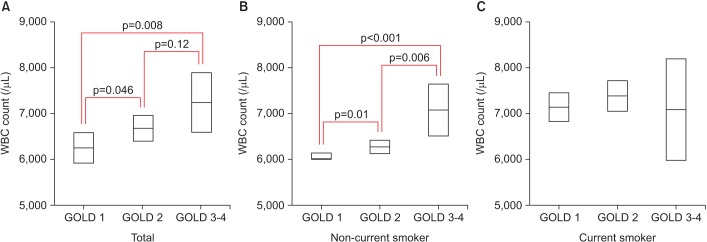
In COPD patients, the WBC count increased according to severity of airflow limitation (6,345±1,769 in GOLD 1, 6,584±1,844 in GOLD 2, 6,833±1,875 in GOLD 3-4; p=0.03) and was higher in current smokers than in non-current smokers (7,231±1,957 in current smoker vs. 6,136±1,631 in non-current smoker; p<0.001). The demographic and clinical characteristics of the COPD were compared according to quartiles of WBC count (Table 1). Quartile (Q) cutoff values were Q1 <5,200, Q2=5,200-6,250, Q3=6,250-7,470, and Q4 >7,470. Sex, waist circumference, smoking status, diabetes, hyperlipidemia, and FVC (L) were significantly different among different quartiles of WBC counts. Proportion of male sex (p for trend <0.001), central obesity (p for trend <0.001), current smoker (p for trend <0.001), diabetes (p for trend <0.001), and hyperlipidemia (p for trend <0.001) increased according to different quartiles of WBC counts. Values of FVC (% predicted) (p for trend=0.01) and FEV1 (% predicted) (p for trend=0.01) decreased according to increase of WBC quartiles. Multivariable analysis for the relationship between degree of airflow limitation and WBC count were performed adjusted for age, sex, waist circumference, hypertension, diabetes, and dyslipidemia. Both the degree of airflow limitation (β=0.10, p=0.002) and current smoking status (β=0.28; p<0.001) were independently associated with the WBC count. Since there existed interaction between severity of airflow limitation and smoking status for WBC counts (p<0.001), we stratified study population based upon smoking status and reanalyzed the effect of degree of airflow limitation on WBC count. WBC counts were significantly different among each COPD stage only in non-current smoker group. WBC counts adjusted by age, sex, waist circumference, hypertension, diabetes, and dyslipidemia were compared according to the degree of airflow limitation and current smoking status in Figure 2.
The relation to WBC count with FEV1 (% predicted) (R=−0.06, p=0.03) were statistically significant, but not with FVC (% predicted) (p=0.06) in COPD patients. Multivariable analysis for the WBC count on lung function was performed after adjustment for age, sex, height, BMI, and current smoking status. The WBC count independently correlated with both decreased FVC (% predicted) and FEV1 (% predicted) (model 1 in Table 2). Even after additional co-variables (presence of hypertension, diabetes, and dyslipidemia) were included to the previous model, the associations between WBC count and lung function were still significant (model 2 in Table 2).
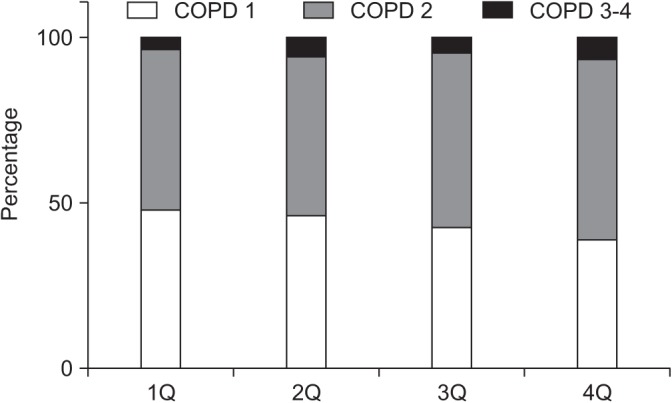
The proportions of patients with the different COPD stages were compared according to quartiles of the WBC count. The associations between the proportions of COPD stage did not reach statistical significant differences according to the quartiles of the WBC count (p=0.07), but showed a tendency to worsen (p for trend=0.008). Progression of the COPD stage was apparent in the fourth quartile (p=0.01 in the post-hoc subgroup analysis) (Figure 3). After stratification by current smoking status, the proportion of COPD stage did not showed significant difference among different quartiles of WBC count (Supplementary Figures S1, S2).
3. WBC count and quality of Life
The relationships between the WBC count and the EQ5D-index or EQ5D-VAS were evaluated. WBC count was not statistically associated with EQ5D-index (p=0.58) or EQ5D-VAS score (p=0.55). Multivariable analysis of the relationship between WBC count and QOL was performed with adjusted for age, sex, BMI, current smoking status, and COPD severity. The WBC count was independently associated with EQ5D-index (p=0.03), but not with EQ5D-VAS score (p=0.41). After further addition of co-variables such as hypertension, diabetes, and dyslipidemia to previous model, the association between WBC count and EQ5D-index was still significant (Table 3).
4. Subgroup analysis according to smoking status
Since smoking status is one of the most important confounders for COPD and since it was shown to have significant influence on the WBC counts in our study, we next stratified the study population according to smoking status. The WBC count correlated with FVC (% predicted) (R=−0.12, p<0.001) and FEV1 (% predicted) (R=−0.10, p=0.003) in the non-current smoker group. However, these correlations were not apparent in the current smoker group (p for FVC [% predicted]=0.56, p for FEV1 [% predicted]=0.52). Multivariable analysis adjusted for age, sex, height, BMI, and current smoking status (model 1), and presence of hypertension, diabetes, and dyslipidemia in addition to model 1 (model 2) resulted in similar outcomes (Table 2). The association between the WBC counts with EQ5D-index was significant only in the non-current smoker group, but not in the current smoker group (Table 3).
Discussion
In this study, a higher WBC count was found to be independently associated with worse FVC (% predicted), and FEV1 (% predicted), and quality of life in COPD patients. These associations were more significant in the non-current smoker group than in the current smoker group. The elevation of the WBC count was independently associated with the COPD severity and current smoking status.
In previous studies, elevation of inflammatory markers, such as the WBC count, CRP, IL-6, and IL-8, had been reported in COPD patients3,4,5,6,7. Singh et al.7 reported that sputum neutrophils showed a weak association with FEV1 (% predicted) (r2=0.025), but not with emphysema or future exacerbation, using data of the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) cohort. However, acquiring a qualified sputum specimen is difficult, and it is necessary to identify reliable biomarker that can be easily measured in the peripheral blood21. Agusti et al.22 compared the characteristics of a population with persistent systemic inflammation using the same ECLIPSE cohort. In this study, COPD patients had a higher WBC count than those of the controls, and groups with increased inflammatory markers showed more exacerbation and higher mortality rate than the groups without increased inflammatory markers. However, the % predicted FEV1 and annual decline rate of FEV1 were not significantly different between the two groups22. In another, smaller study by Fattouh and Alkady23, the authors also reported increased exacerbation in the high WBC group, whereas no significant correlation between the % predicted FEV1 and WBC count was observed. Unlike the risk of exacerbation, the correlation between the peripheral WBC count and lung function has been reported to be mainly insignificant.
Our study revealed that this insignificant correlation between WBC count and lung function in previous reports were attributable to effect of smoking status. Values of WBC count are related to both lung function and QoL which determine COPD stage. Therefore, WBC count can be used as indicator for COPD severity, especially in non-current smoking COPD patients. The interaction between smoking status and COPD stage on WBC count might be result from effect of smoking on COPD.
Furthermore, COPD patients frequently have comorbidities related to systemic inflammation including metabolic syndrome, and elevation of these biomarkers could be consequences of other coexisting disease9, not by COPD itself. To discriminate their confounding effects and clearly identify their relationship with COPD, we examined the correlations of the WBC count with the severity of COPD, adjusting for hypertension, diabetes, dyslipidemia, and other confounding factors in a sufficient number of patients.
Therefore, the WBC may represent a powerful biomarker for COPD patients, as it correlates to lung function and QoL, in addition to the risks of exacerbation and mortality.
Although this study identified independent relationships between the WBC count and COPD severity, the following limitations of the study should be noted when interpreting these results: first, we could not obtain data of other inflammatory markers, the diffusing capacity for carbon monoxide, emphysema index, or objective functional status measurements, such as the 6-minute walk distance. Second, we used the EuroQoL instead of the CAT score for measuring QoL, which is a generic questionnaire, although it has been reported to show a good correlation with the SGRQ score17,18. Third, we did not evaluate post-bronchodilator FEV1 and FVC, which are commonly used as lung function parameters in COPD patients, as this study was part of the national health survey. Fourth, differential leukocyte count or changes of WBC counts during follow-up or exacerbations could not be evaluated since this study was part of national survey. Fifth, WBC counts can be also influenced by infectious, rheumatologic, hematologic, or malignant diseases other than metabolic diseases. Though number of these population were small, our study could not exclude all these population, so WBC count could be influenced by these comorbidities. Fifth, number of advanced COPD patients included in our study were relatively small than that of COPD I-II patients, therefore caution is required in interpreting these results. Lastly, we could not completely differentiate COPD from asthma. Although KNHANES includes a self-reported questionnaire for asthma, many patients may not be able to differentiate these diseases accurately. Therefore, chronic smoking-related asthma or asthma-COPD overlap syndrome may have existed in our study population, and this relation could be different in this subgroups. Further large trials evaluating the effect of the WBC count on the annual decline rate of lung function, functional capacity, and/or mortality are needed to confirm our findings.
In conclusion, elevation of the WBC count is independently associated with current smoking status and COPD severity. A high WBC count is a related to poorer lung function and lower quality of life in COPD patients, especially in non-current smokers. Based on our result, the WBC count could potentially be used as a powerful prognostic biomarker for COPD patients.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Supplement1
Supplement1 Print
Print Download Citation
Download Citation






