



Introduction
Bronchiectasis is a chronic airway disease characterized by a clinical syndrome that includes cough, sputum production, hemoptysis, and bronchial infection. Radiographic images illustrate permanent dilatation and a thickened wall of the bronchi [1]. Bronchiectasis is increasing in prevalence and escalates the public health burden, resulting in increased health care costs, hospitalization rates, and mortality [2,3]. A recent study in Korea using a government health insurance database showed that the prevalence of bronchiectasis in Korea was higher than that in other Western countries, and the healthcare cost was high [4]. In addition to the high prevalence and economic burden, assessment of health-related quality of life (HRQOL) is important in chronic diseases such as bronchiectasis, as it can evaluate the overall impact on health from the patientŌĆÖs point of view. HRQOL is severely impaired in bronchiectasis [5]. The health status of bronchiectasis patients can be evaluated with validated questionnaires, such as the St. GeorgeŌĆÖs Respiratory Questionnaire (SGRQ), Leicester Cough Questionnaire, and Quality of Life-Bronchiectasis (QoL-B) [6-8]. However, these questionnaires are not practical for general use in the management of bronchiectasis patients as they are too lengthy, and the scoring system is very complicated. Spinou et al[9]. recently developed a shorter and more practical tool, termed the Bronchiectasis Health Questionnaire (BHQ). Despite the questionnaireŌĆÖs simplicity, the authors concluded that the questionnaire works well in a different population from the development cohort. The authors also presented a translation of the questionnaire into 11 languages with linguistic validation [9]. Given the significance of the health impact of bronchiectasis in Korea, we need a tool for assessing HRQOL of Korean patients with bronchiectasis.
In the present study, we report on the process of the development of the Korean version of the BHQ (K-BHQ) using a standardized methodology. We also evaluated the validity of the K-BHQ in Korean patients with bronchiectasis.
Materials and Methods
1. Study subjects
Patients with stable bronchiectasis were enrolled from two academic hospitals, the Hanyang University Hospital and the Asan Medical Center, Seoul, Korea. These patients were a part of a patient cohort from an ongoing study, the Korean Multicenter Bronchiectasis Audit and Research Collaboration (KMBARC) [10]. The candidates for enrollment in the KMBARC study were patients in stable condition with bronchiectasis confirmed by chest computed tomography. Baseline clinical information, including the modified Medical Research Council (mMRC) dyspnea scale score, lung function, and exacerbation history, was obtained in addition to the K-BHQ and Korean version of the Chronic Obstructive Pulmonary Disease Assessment Test (K-CAT) scores.
2. Methods
1) BHQ translation from English into the Korean language
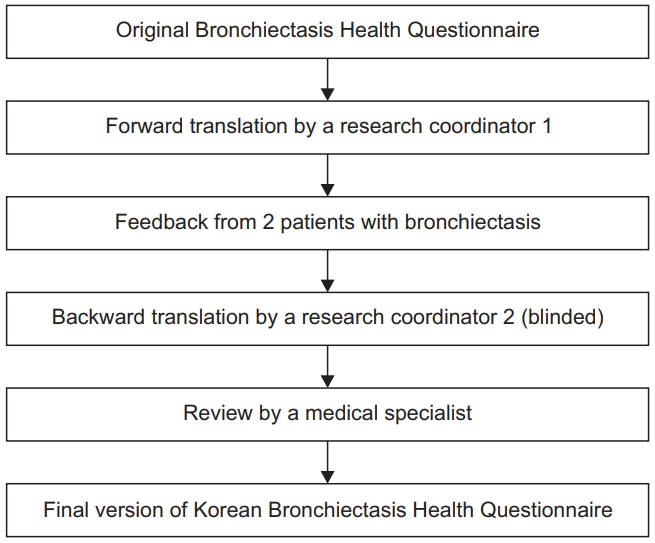
We obtained permission for the copyright using the original version of the BHQ from Dr. Surinder Birring of KingŌĆÖs College Hospital, UK. A research coordinator performed the 1st translation of the original version of the BHQ into the Korean language with the aid of the Google Translator. The research coordinator obtained feedback regarding the 1st translation version from two Korean patients with bronchiectasis. The two patients understood the meaning of all translations, except for the meaning of the translation for question 4 which read; ŌĆ£In the last 14 days, my chest has felt clear.ŌĆØ For question 4, we revised the translation with the addition of a popular word in parentheses. Another coordinator translated the revised version of the Korean language back into English. She was blinded to the original English expression of the BHQ. The questionnaire that was translated back into English was reviewed by the developer, Dr. Surinder Birring. One of the authors in this study compared the questions of the original version with those of the back-translated version in English (Figure 1). The final version of the K-BHQ is given in the Supplementary Material.
2) K-BHQ validation
The validity was assessed by investigating the relationship between the K-BHQ scores and K-CAT scores. We also investigated the relationship between the K-BHQ scores and other variables of the mMRC dyspnea scale, lung function, and exacerbations.
3) Statistical analysis
To evaluate the validity of the K-BHQ, correlation analysis was conducted using PearsonŌĆÖs correlation coefficient (r) for the parametric variables and SpearmanŌĆÖs correlation coefficient (Žü) for the non-parametric variables.
Statistical analysis was performed using SPSS for Windows version 18.0 (SPSS Inc., Chicago, IL, USA). All data are expressed as means and standard deviations (SD) or frequencies. Statistical significance was accepted for p-values less than 0.05.
4) Ethics statement
Approvals were obtained from the institutional review boards (IRBs) of the Asan Medical Center and the Hanyang University Hospital for patient data collection as a component of the cohort study of the KMBARC (IRB No. 2020-0087, 2018-0691). Written informed consent was obtained from all participants. For this study, we obtained approval from the IRB of the Asan Medical Center.
Results
1. Patients
A total of 126 patients with bronchiectasis were included. The mean (┬▒SD) age was 64.3┬▒9.7 years, and 53.2% of the patients were women. Sixty percent of the patients had never smoked, and 38% had a history of tuberculosis. The mean (┬▒SD) forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were 60┬▒19% and 72┬▒17% predicted values, respectively. Most patients did not experience exacerbations or hospitalizations (Table 1).
2. Correlation between K-BHQ and other clinical measurements
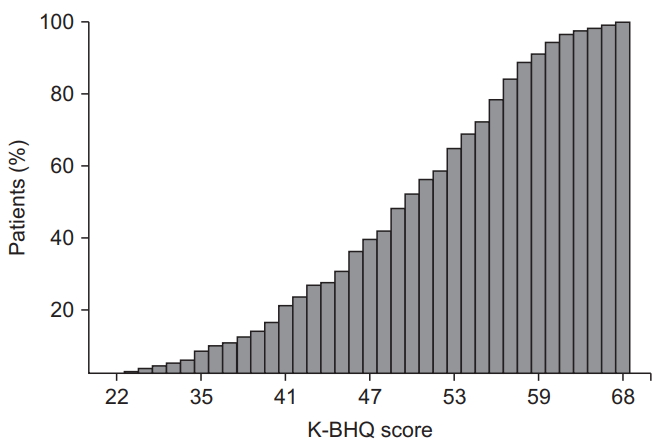
The mean (┬▒SD) K-BHQ total score was 49.0┬▒9.1. The scores were evenly distributed from the mean (Figure 2). The correlation between the K-BHQ scores and the K-CAT scores was good (r=-0.656, p<0.001) (Figure 3). The K-BHQ score correlated moderately with the mMRC dyspnea scale (Žü=-0.409, p<0.001) (Figure 4), FEV1 % predicted (r=0.406, p<0.001), and FVC % predicted (r=0.351, p<0.001) (Figure 5) and weakly correlated with the number of exacerbations requiring hospitalization in the past year (Žü=-0.303, p=0.001) and any exacerbations (Žü=-0.245, p=0.006) (Figure 6, Table 2).
Discussion
The K-BHQ is a translated version of the original BHQ, which is a brief, practical, and well-validated questionnaire for assessing the HRQOL of patients with bronchiectasis in English. This study described the process of translation and demonstrated that the K-BHQ scores correlated strongly with the K-CAT scores and moderately with mMRC dyspnea scale scores, lung function, and exacerbations requiring hospitalization. These results suggest that the K-BHQ is valid for assessing the HRQOL or health status in Korean patients with bronchiectasis.
Although the prevalence of bronchiectasis is high in Korea [4], there is no tool to properly assess the health status of bronchiectasis patients. A previous study showed that the K-CAT developed for chronic obstructive pulmonary disease (COPD) patients is valid for Korean patients with bronchiectasis [11]. The CAT is a tool for patients with COPD; however, there is no item for hemoptysis, which is a symptom specific to bronchiectasis. In addition, the CAT does not cover the bacterial infection that is common in patients with bronchiectasis. Therefore, we translated the original BHQ developed in British English into Korean and evaluated the validity of the K-BHQ for assessing the HRQOL of patients with bronchiectasis.
The QoL-B is another validated bronchiectasis-specific health status questionnaire [5,12]. The QoL-B has 37 items and 8 domains, while the BHQ consists of 10 items and does not provide an overall quality of life score. The BHQ may, therefore, be more appropriate for clinical and research settings where the implementation of a simple questionnaire is an important practical factor, and when a single score is preferable in order to easily interpret clinical outcomes.
The translation process was based on linguistic validation. Linguistic validation is a series of processes designed to ensure that translations are linguistically accurate, culturally appropriate, and reviewed by experts in the field. The good translation goes beyond simply changing words or word order. Many semantic and cultural specifications must be considered [13]. As much as possible, we attempted to carry out our translation in a manner that reflected the development of the original questionnaire. During the translation process, we were in correspondence with the author of the original BHQ study. The translation proceeded in the following order: (1) indepth analysis of the original wording and suggestions for suitable translation alternatives, (2) a forward/backward translation step, (3) review of the back translation by the developer, and (4) review of the translated questionnaire by a respiratory clinician fluent in the language [9].
Compared with the original BHQ, the K-BHQ showed lower convergent validity (r=-0.82 vs. r=-0.66). This is probably because the validity of the original BHQ study was obtained using the SGRQ, while validation in this study was conducted using the K-CAT. The K-BHQ scores are more closely correlated with lung functions and less correlated with exacerbations and hospitalizations than the original BHQ. The reason may be due to differences in patient characteristics. Patients enrolled in the K-BHQ study were older and had lower lung functions, less exacerbations, and more history of tuberculosis than the BHQ study participants.
In addition, a recent correlation study of quality of life in bronchiectasis reported a correlation between CAT and BHQ scores and showed similar results to the correlation between K-BHQ and K-CAT in this study [14].
In summary, the K-BHQ is a simple, practical, and well-validated questionnaire for assessing health status in Korean patients with bronchiectasis.




 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Supplement
Supplement Print
Print Download Citation
Download Citation






