


Introduction
Tracheostomy is a common surgical procedure in the intensive care unit (ICU) for patients requiring prolonged mechanical ventilation. Theoretically, a tracheostomy has some advantages over a translaryngeal endotracheal tube for respiratory physiology, nursing care, and psychology1,2. Although some beneficial effects of early tracheostomy have been reported3, recent large studies were unable to show a reduced incidence of ventilator-associated pneumonia (VAP) and ICU mortality in patients with an early tracheostomy compared to those with a late tracheostomy4,5. Despite that it is a common procedure, the optimal time for a tracheostomy in the ICU is not yet clearly defined1. Furthermore, the selection of patients and timing of the decision for a tracheostomy are subjective, as no reliable tests have been established to predict the need for prolonged ventilation.
Intubation for 2 weeks is considered safe with the use of a low-pressure and high-volume endotracheal tube cuff6. According to nationwide surveys, a tracheostomy was performed within 14 days in 90% of German ICUs7 and within 21 days in 68% of French ICUs8. The criterion for an early tracheostomy in clinical trials was defined from as early as 48 hours3 to as late as 8 days5.
Traditionally, 2 weeks was the time limit to make the decision for a tracheostomy in all patients requiring prolonged mechanical ventilation. The timing of a tracheostomy is diverse, and delaying a tracheostomy for more than 2 weeks is not uncommon in the ICU, but the reasons for such a delayed tracheostomy have not been investigated. This study was performed to determine the exact timing of a tracheostomy and factors influencing tracheostomy timing in the medical ICU of a tertiary referral hospital in Korea.
Materials and Methods
1. Study population
Patients who were admitted to the medical ICU (22 beds) of Seoul National University Hospital from January 2008 to December 2009 were recruited. Inclusion criteria were age >18 years, mechanical ventilation with translaryngeal intubation and first tracheostomy. Exclusion criteria were postoperative patients, multiple separate ICU admissions during the same hospital stay and uncontrolled or haematological malignancy. This protocol (H-1006-141-322) was approved by the Seoul National University Hospital Institutional Review Board.
2. Assessment of organ failure
Organ failure was defined as a Sequential Organ Failure Assessment (SOFA) score9Ōēź2 on each item, as follows: PaO2/FiO2<300 mm Hg, the use of inotropics or vasopressors, platelets<100,000/mm3, bilirubinŌēź2.0 mg/dL, creatinineŌēź2.0 mg/dL and Glasgow Coma ScaleŌēż12. The development of organ failure was defined as the existence of the above criteria from ICU admission to the day of the tracheostomy.
3. Statistical analysis
p-values were calculated using the Žć2 test or Fisher's exact test for categorical variables and the Mann-Whitney U-test for continuous variables. Odds ratios (ORs) were calculated from the logistic regression model in the multivariate analysis. A p<0.05 was considered to indicate statistical significance. STATA version 11.0 (StataCorp., College Station, TX, USA) was used for the analysis.
Results
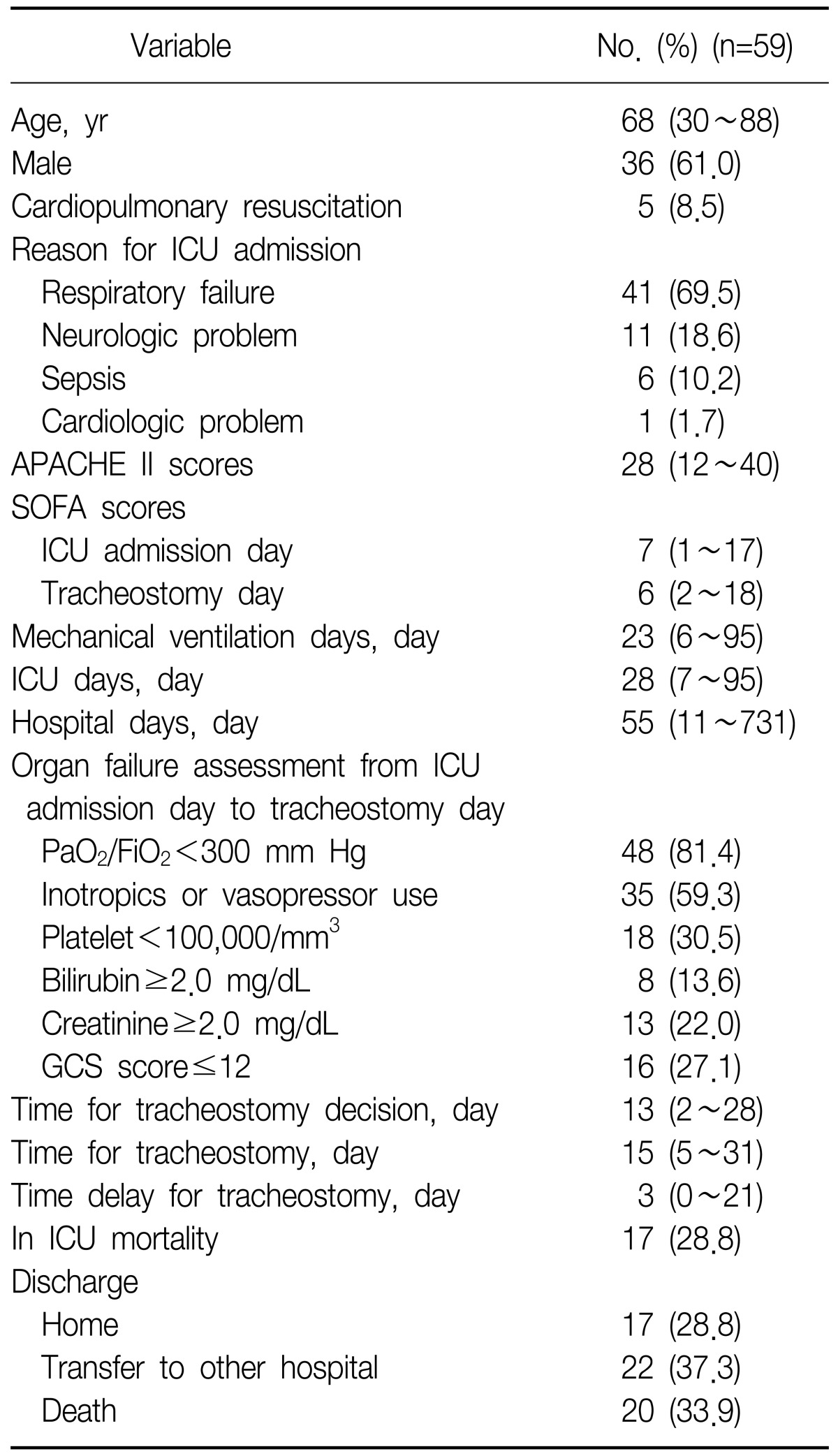
Fifty-nine patients were included in the study (Table 1). The median age of the patients was 68 years (range, 30~88 years), and male gender was predominant (61.0%). The common causes of medical ICU admission were respiratory failure (69.5%) and neurological problems (18.6%), sepsis (10.2%) and cardiac problems (1.7%). Cardiopulmonary resuscitation (CPR) was performed in five of 59 patients prior to medical ICU admission. Median Acute Physiology And Chronic Health Evaluation (APACHE) II score10 and SOFA score on ICU admission day were 28 (range, 12~40) and 7 (range, 1~17), respectively. The patients were given mechanical ventilation support for 23 days (range, 6~95 days) and remained in the medical ICU for 28 days (range, 7~95 days). Under mechanical ventilation support, the decision to perform a tracheostomy was performed on day 13 (range, 2~28 days) and the actual bedside operation was done on day 15 (range, 5~31 days). The time delay for tracheostomy was 3 days (range, 0~21 days).
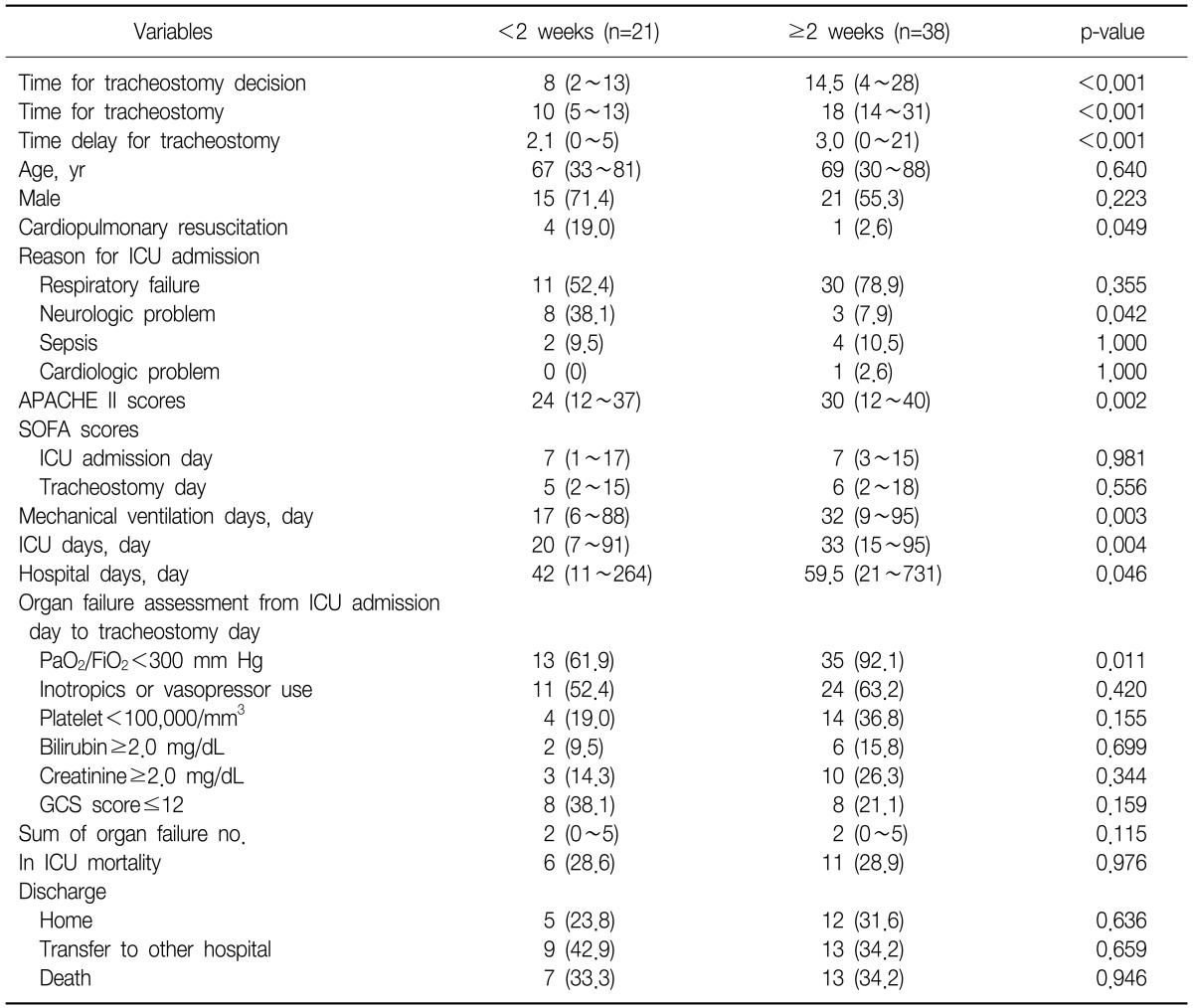
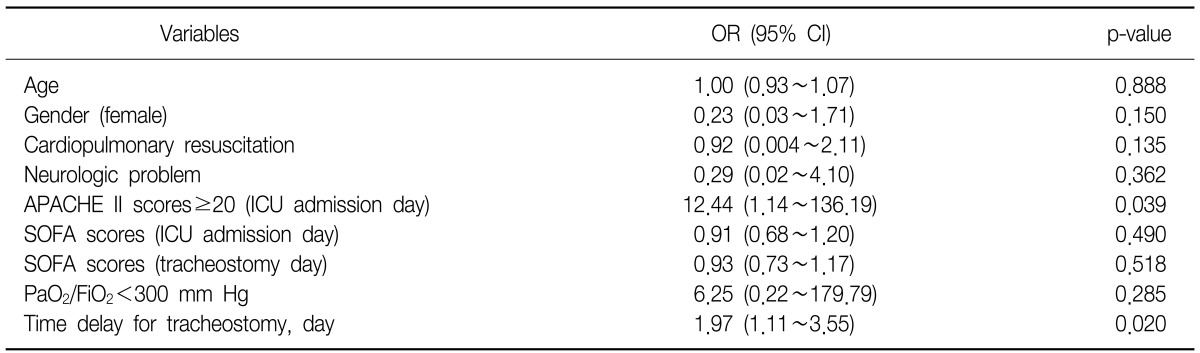
Patients were grouped according to the day of tracheostomy, i.e., whether it was performed before or after 2 weeks. Among the 59 patients, 21 (35.6%) received a tracheostomy before 2 weeks (group I), and 38 (64.4%) received one after 2 weeks (group II) (Table 2). In the univariate analysis, the decision and operation time of the tracheostomy were significantly different between the two groups. The time delay for tracheostomy was also different between group I and group II. Compared with group II, group I showed more frequent CPR (19% vs. 2.6%, p=0.049), more common neurological problems (38.1% vs. 7.9%, p=0.042) and lower APACHE II scores (24 vs. 30, p=0.002). In the assessment of organ failure, group II patients showed a higher frequency of PaO2/FiO2<300 mm Hg (61.9% vs. 92.1%, p=0.011). Table 3 shows the multivariate analysis for a tracheostomy after 2 weeks. Our data revealed that higher APACHE II score (Ōēź20) (OR, 12.44; 95% confidence interval [CI], 1.14~136.19; p=0.039) and time delay for tracheostomy (OR, 1.97; 95% CI, 1.11~3.55, p=0.020) were independent significant factors for performing a tracheostomy after 2 weeks.
Discussion
Early prediction of patients who will eventually need a tracheostomy is very difficult. The time for a tracheostomy varies, and the optimal time has not been established. Dunham and LaMonica6 reported that endotracheal intubation for up to 2 weeks is not associated with increased complications related to translaryngeal intubation. The consensus conference recommends performing a tracheostomy after 3 weeks of translaryngeal intubation11. Compared to this relatively late tracheostomy, recent studies have shown a clinical benefit of an early tracheostomy4,5,12,13. Some studies have shown that early tracheostomy was related with early weaning from mechanical ventilation; however, a large randomised controlled trial failed to demonstrate a reduction in VAP and mortality through the use of an early tracheostomy5.
According to our results, the median decision time for a tracheostomy was 13 days, and a tracheostomy was performed at day 15 after translaryngeal intubation. Compared to recent clinical trials, this could be considered a late tracheostomy. Some possible explanations for this include the following. First, the standardised tracheostomy protocol and early-tracheostomy decision algorithm may be helpful. The objective decision algorithm for a tracheostomy predicts prolonged ventilation more effectively14, whereas the standardised protocol for a tracheostomy may minimise clinical variation15. Second, the time gap between decision-making and the actual operation of the tracheostomy was 3 days. Furthermore the time delay for tracheostomy was significantly different between group I and group II. This meant that 3 days were needed for interdepartmental consultation with otolaryngologists and surgical preparation for the tracheostomy and as the time delayed more, the actual tracheostomy was performed lately. As the standard method for a tracheostomy was a bedside surgical procedure at that time in our hospital, the time gap was inevitable. After recently introducing percutaneous dilatational tracheostomy in our medical ICU, we have been able to successfully shorten the gap.
We found some similar patterns in the decision-making concerning tracheostomy. Most of the patients who were assessed with an irreversible brain injury (previous neurological problems or post CPR) received an early (<2 weeks) tracheostomy (Table 2), while patients who had higher APACHE II scores received a late (Ōēź2 weeks) tracheostomy. If high mortality was expected on the day of medical ICU admission, the decision and procedure time for the tracheostomy were delayed. Also, a late tracheostomy was preferred in the event of respiratory failure (PaO2/FiO2<300 mm Hg).
Effects of a selection bias may exist due to the retrospective nature of this study. According to our results, the median time of tracheostomy was 15 days after endotracheal intubation. The patient must be alive at the time with tolerable operative conditions to receive a tracheostomy. If a patient showed unfavourable operative conditions, the tracheostomy might have be postponed. During these delays, the critically ill cases may have died before a tracheostomy. In other words, only those who survived longer in the medical ICU received a tracheostomy. Considering this selection bias, we did not compare the mortality according to the timing of the tracheostomy.
In conclusion, tracheostomy was performed a median of 15 days after endotracheal intubation in the medical ICU. Our data suggest that high APACHE II scores (Ōēź20) may influence the timing of a tracheostomy in a medical ICU. And the time gap caused by interdepartmental consultation for tracheostomy was another independent factor for delayed tracheostomy.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






