



Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease that is characterized by the chronic and persistent obstruction of small and medium airways. This disease is mainly caused by exposure to tobacco smoke, occupational exposure, and biomass combustion [1-3]. It is related to high rates of morbidity and mortality [2,4], especially when individuals have other associated concomitant diseases, such as cardiovascular ones [5].
Cardiovascular comorbidity is common in individuals with COPD due to smoking, in addition to other shared risks that include genetic susceptibility, systemic inflammation, and aging [6]. In recent years, systemic inflammation has been increasingly recognized as an important common pathway for both conditions [7]. This inflammation, expressed by increased levels of cytokines, such as tumor necrosis factor ╬▒, interleukin-1 (IL-1), and IL-6, can accelerate and perpetuate disease progression and exacerbations of both diseases [8]. Furthermore, evidence indicates that individuals with COPD and concomitant heart disease have a worse prognosis, compared to subjects with only COPD, and is associated with higher mortality [1,9].
Other factors can contribute to the occurrence of compromised cardiac function in the disease. Individuals with this disease seem to have a larger left ventricular mass, which impacts their survival [10]. The pulmonary hyperinflation characteristic of the disease can cause cardiac compression, reducing both the left ventricle and the atrium filling, even in the absence of increased pulmonary arterial pressure [11,12]. These conditions can be aggravated by the negative effects of hypoxemia on diastolic filling [13].
These factors promote a high prevalence of cardiovascular comorbidities, which interferes with the choice of therapeutic interventions, including pharmacological treatment. The use of ╬▓-blockers has been proposed for their known cardioprotective effects, in addition to reducing heart rate, and improving systolic and diastolic dysfunction. However, due to adverse reactions, and the risk of causing bronchospasm, there is reluctance to use them. One of the key issues regarding the more widespread use of ╬▓-blockers in COPD is the concern with ╬▓2 receptor antagonism and associated airway smooth muscle constriction, which can occur even with cardioselective agents that exhibit preferential ╬▓1 blockade, leading to a worsening of lung function, especially in more severe cases with compromised respiratory reserve [14].
As a result, through current scientific evidence, researchers have sought to investigate the effects of the use of these drugs in COPD, especially in terms of disease severity, exacerbations, and mortality. However, the articles that address this issue are heterogeneous, carried out in populations with specific characteristics, who use different classes and doses of ╬▓-blockers, and consequently present different results. Therefore, a current systematic review of these studies is necessary to resolve the present differences, understand the effects of these drugs on different outcomes, and finally, contribute to decision-making.
Thus, the aim of the present study is to summarize the existing evidence on the effects of the use of ╬▓-blockers in COPD associated with cardiovascular comorbidities in relation to the outcomes of disease severity, exacerbations, and mortality.
Materials and Methods
This is a systematic review and metanalysis study carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Recommendation (Main Items for Reporting Systematic Reviews and Meta-analysis) [15]. The following databases were used: EMBASE, Medical Literature Analysis and Retrieval System Online (Medline), Latin and Caribbean Literature of Sciences de la Health (Lilacs), and Scientific Electronic Library Online (Scielo), Cochrane Library, and Science Direct. The collection was carried out from June 2023 to January 2024.
The elaboration of this research was structured based on the PICOS strategy, an acronym for Population (individuals with COPD and cardiovascular diseases), InterventionŌĆöor Exposure, for observational studies (use of ╬▓-blockers), Comparison (cardioselective and non-selective), Outcomes (severity of the disease, exacerbations, and mortality), and Study design (observational studies) [16]. The keywords and synonyms were used according to the databases: ŌĆ£Pulmonary Disease, Chronic Obstructive; Cardiovascular Diseases; Severity of Illness; Disease exacerbation; Mortality; Adrenergic beta-antagonists,ŌĆØ identified in the DeCS vocabulary system (Descritores em Ci├¬ncias da Sa├║de [Health Sciences Descriptors]), the Medical Subject Headings (MeSH), and Embase Subject headings (Emtree), using the Boolean operators ŌĆ£ANDŌĆØ and ŌĆ£OR.ŌĆØ The search was performed using the words found in the titles, subjects, and abstracts of the articles.
Observational studies were included in which the effects of ╬▓-blockers in individuals with a diagnosis of COPD (confirmed by spirometry) and cardiovascular comorbidities were included, and related to the outcomes of disease severity, exacerbations, or mortality. Studies should present the odds ratio (ORs) or mean and standard deviation and their corresponding confidence intervals (CI), or sufficient data to calculate these parameters.
Studies that did not present important characteristics of the sample, such as age and disease severity (data that could interfere with the results), were excluded; as were articles that did not present relevant information about the pharmacological treatment, such as the medication used. The selection process, data extraction from the articles, and identification of methodological aspects was carried out by two independent reviewers. When there was disagreement between them, the reviewers read the article again for re-evaluation. If the disagreement persisted, a third independent reviewer would assess and make the final decision.
1. Statistical analysis
Subgroup analysis was performed according to the outcomes studied: disease severity, exacerbations, and mortality. For the mortality and exacerbations outcomes, a random effect model was used; while for the disease severity outcome, the mean and standard deviation were used. Data were graphically displayed using forest plot. A p-value less than 0.05 was considered statistically significant.
Statistical heterogeneity between studies was assessed using the Cochrane Q test and the I2 inconsistency test. The following cutoff points were adopted: 0% to 25%: mild heterogeneity, acceptable; >25% to 50%: moderate heterogeneity; >50%: high heterogeneity [17]. Sensitivity analysis was evaluated using the Jackknife procedure, examining the individual influence of each study.
The quality of included studies was assessed using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies from the National Heart, Lung, and Blood Institute (NHLBI). The assessment of methodological quality was performed by two independent researchers. A third evaluator measured the inconsistencies, and made the final decision. Funnel charts were generated to assess publication bias. Statistical analysis were performed using Review Manager version 5.0 (Cochrane Collaboration, London, UK).
The protocol of the construction steps of this systematic review was published in the International Prospective Register of Systematic Reviews (PROSPERO), under registration CRD42020155656.
Results
The search in the databases resulted in 24,283 articles (Medline: 19,985; EMBASE: 3,264; Science Direct: 1,029; Lilacs: 2; Scielo: 1; Cochrane Library: 2), leaving 24,256 records after removing the duplicates. Of these, 61 articles were selected by title tracking; 22 were excluded due to the abstract not meeting the selection criteria, leaving 39 articles for full reading. Of these, it was found that 19 of them did not meet all the inclusion criteria, resulting in the final selection of 20 articles, as shown in Figure 1.
The 20 articles were read analytically and selectively, and organized into two tables with relevant research information, such as characteristicsŌĆöauthor, year; type of study (duration); data source (country); sample (follow-up); and cardiovascular comorbidity (Table 1) [18-37], and the analysis of the studiesŌĆötype of ╬▓-blocker used, outcomes, and results, as shown in Table 2.
Of the 20 articles, most were cohort studies, 15 being retrospective [18-23,26-28,30,32-34,36,37], and three prospective [24,31,35]. Only one article was cross-sectional observational [25], and one case-control [29]. In total, 237,709 individuals participated in the 20 surveys. For data collection [16], articles used secondary data from medical records and multicenter research banks [18-23,26-28,30,32-35,37], while four used primary data [24,25,31,36].
Of the 20 articles, 14 studies evaluated the outcome mortality [18-24,26-28,32,33,35,37]; 14, exacerbations [18,19,21,23-25,27,29,32,34,36,37]; and four, disease severity, according to the spirometric data [19,25,30,31]. The comorbidities studied by the studies are: congestive heart failure (CHF) [18-23,25,26,28-30,33-37]; systemic arterial hypertension [18,21-30,34,37]; cerebrovascular disease [19,22,23,26,29,32,34]; arrhythmia [23,29,32-35]; ischemic heart disease [21,28,39,32-34]; atrial fibrillation [27,30-32,37]; coronary artery disease (CAD) [24,25,30,35,37]; acute coronary syndrome [18]; and abdominal aortic aneurysm [31]. Table 3 shows the ╬▓-blockers.
1. Mortality
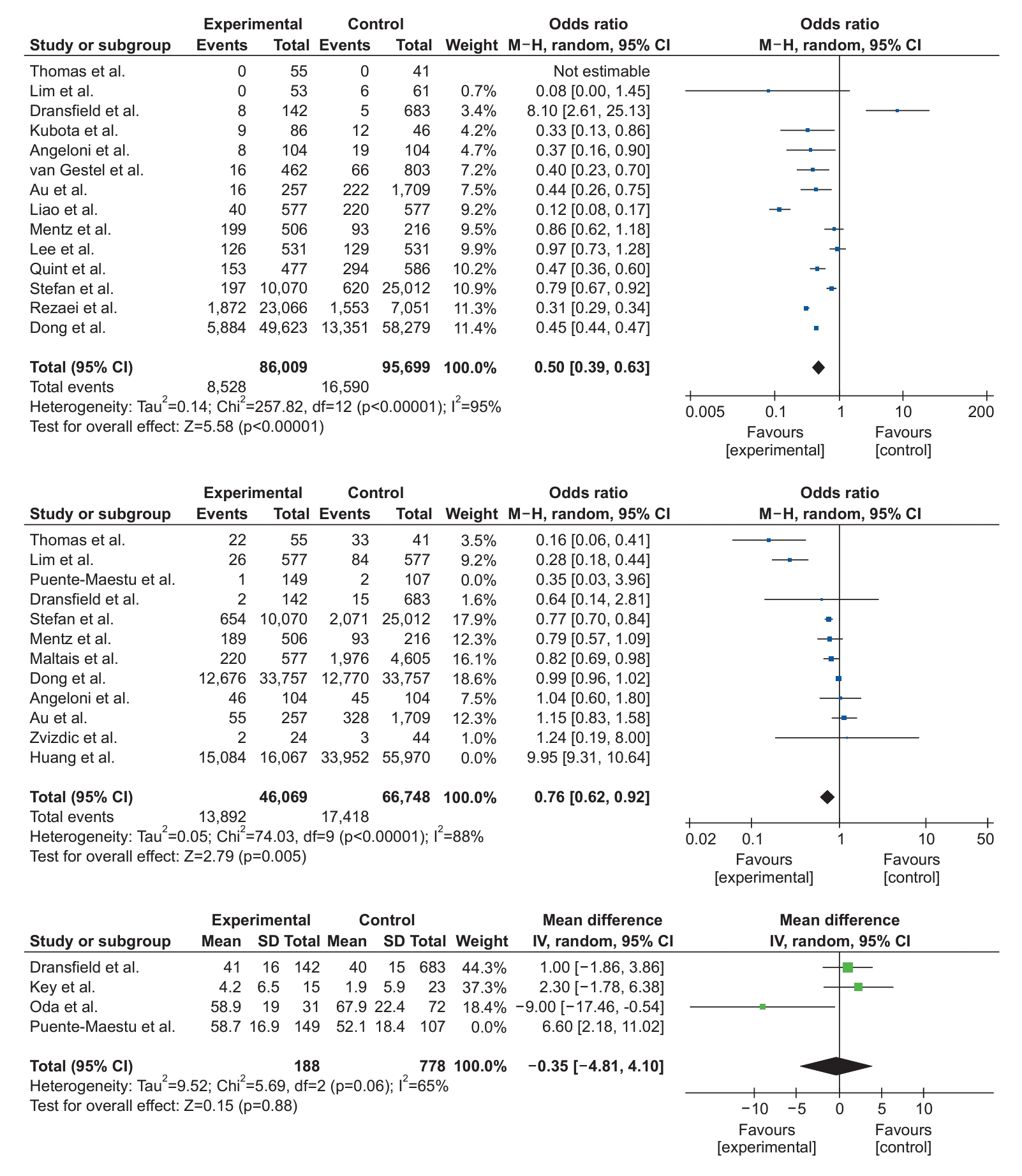
The OR for the mortality outcome was 0.50 (95% CI, 0.39 to 0.63; p<0.00001), which was favorable to the group that used ╬▓-blockers. The results indicate a high degree of heterogeneity among the included studies (I2=95%) (Figure 2).
2. Exacerbations
The OR for the exacerbation outcome was 0.76 (95% CI, 0.62 to 0.92; p=0.005), which was favorable for the group that used ╬▓-blockers. The results indicate a high degree of heterogeneity among the included studies (I2=88%) (Figure 2). Data from the studies by Puente-Maestu et al. [25] and Huang et al. [29] were not included in the analysis, because they had other study designs, which interfered with the result, and led to a greater degree of heterogeneity (I2=100%).
3. Disease severity/severity of illness
Effects on disease severity were assessed using mean difference with 95% CIs using a random-effects model. The aggregated results of these studies suggest that there is no statistically significant association between the use of ╬▓-blockers and COPD severity (difference between means=ŌłÆ0.35; 95% CI, ŌłÆ4.81 to 4.10; p=0.8). The results indicate a high degree of heterogeneity among the included studies (I2=65%) (Figure 2). Data from the study by Puente-Maestu et al. [25] were not included in the analysis because of a different study design, which interfered with the result, and led to a greater degree of heterogeneity (I2=73%).
All 20 articles finally selected presented the research question or objective clearly, specified the population, and showed a participation rate of eligible people of at least 50%. All study participants were selected and recruited from similar populations with pre-specified selection criteria. Only one study [36] did not provide a justification for the sample size. The article by Puente-Maestu et al. [25] was the only cross-sectional study, so it was not applicable to analyze whether the exposures of interest were evaluated before the result; whether there was enough time for an association between exposure and outcome; if exposure was evaluated more than once over time; and if there was loss to follow-up.
Across the 20 studies, different levels of exposures were examined, and exposure and outcome measures were clearly defined, valid, reliable, and consistently implemented, but only one study [34] reported blinding to the exposure status of participants. The main variables were measured and statistically adjusted for their impact on the relationship between exposure and outcome in all studies, as shown in Table 4.
Discussion
The results of the present systematic review and meta-analysis suggest that ╬▓-blockers have positive effects on mortality [18,19,22-24,35], and exacerbation [18,19,23,24,29,36], outcomes, compared to the results of individuals who did not use them. For the severity of the disease, there was a reduction in pulmonary function in subjects with COPD [30,31].
1. Mortality
Regarding the mortality outcome, studies have shown that the use of ╬▓-blockers in individuals with COPD is associated with a reduction in the number of deaths from all causes. Compared to the use of calcium channel blockers, all ╬▓-blocker dosage levels were related to lower mortality. It is supposed that the apparent benefit of these medications may be related to the reduction of cardiovascular events [18,19].
In addition to this apparent protective effect of ╬▓-blockers, according to Dransfield et al. [19], treatment with short-acting ╬▓-agonists is associated with a reduction in mortality. For the authors, it is possible that this result reflects the avoidance of administering short-acting ╬▓-agonists among subjects with a higher risk of death, such as those with tachyarrhythmia or other unstable heart disease, rather than a true beneficial effect among the recipients [19]. Other researchers found that ╬▓-agonists did not modify the effects of ╬▓-blockers on mortality [18].
In addition, Quint et al. [22] found that individuals who did not use ╬▓-blockers after myocardial infarction were more likely to use inhalers for COPD. Previous research carried out in animal models has shown that ╬▓-blockers can up-regulate ╬▓2 receptors in the lung, and thus improve the responsiveness and efficacy of inhaled bronchodilators and ╬▓2-sympathomimetics [24,38].
At first sight, this effect seems to be a counter-intuitive way through which the ╬▓-blocker can exhibit beneficial effects, but the possibility is that the up-regulation of ╬▓2 receptors by chronic ╬▓-blockade can improve the efficacy of ╬▓2-agonists [39]. This pathway is still valid regardless of selectivity, because drugs such as atenolol and bisoprolol have been shown to exert significant ╬▓2 adrenergic receptor antagonism, even at therapeutic doses, which can result in the up-regulation of ╬▓2-adrenoceptors [24,40].
Stefan et al. [21] found the ╬▓1 blocker selectivity to be associated with the risk of mortality, while non-selective ╬▓-blockers were associated with an increased risk of readmission. These findings corroborate data from previous studies that found that non-selective ╬▓-blockers increase hospital admissions in individuals with COPD, decrease forced expiratory volume in 1 second (FEV1), and may inhibit the bronchodilator response to ╬▓2 agonists [21,41]. However, another article found no significant difference between cardioselective and non-selective ╬▓-blockers for 60-day mortality [23].
Regarding the specific type of ╬▓-blocker, Su et al. [42] demonstrated a significantly better dose-dependent survival outcome associated with the use of bisoprolol in individuals with CHF and COPD, whereas metoprolol and carvedilol showed no difference in survival. Non-selective ╬▓-blockers have been found to reduce FEV1 and the effect of bronchodilator treatment, in addition to increasing airway hypersensitivity in individuals with COPD [42,43].
However, the use of metoprolol also showed no survival benefit. As a selective ╬▓1 blocker, metoprolol has been shown to increase airway hyperresponsiveness in subjects with COPD, whereas celiprolol, another selective ╬▓-blocker, has shown no negative pulmonary effect. These findings suggest that pulmonary influences differ between ╬▓-blockers, some of which continue to have a potential negative pulmonary effect [42,43].
2. Exacerbations
Regarding the exacerbation outcome, Su et al. [42] found that individuals who used ╬▓-blockers had a point estimate of fewer exacerbations than those who did not use it. For the authors, potential biological and non-biological explanations may include the up-regulation of ╬▓ receptors and better response to bronchodilators associated with ╬▓-blocker use, or the influence of pulmonary disease severity on ╬▓-blocker prescription practices [44,45].
Dransfield et al. [19] corroborate these findings by observing a trend toward a reduction in COPD-related hospitalizations among those using ╬▓-blockers. However, compared to individuals treated with a selective ╬▓1 agent, subjects treated with a non-selective ╬▓-blocker had a 25% chance of readmission within 30 days [21]. But Mentz et al. [23] found no evidence that ╬▓-blocker selectivity interfered with readmission.
Huang et al. [29] found that individuals with COPD who received selective ╬▓-blockers had a lower risk of severe exacerbations, especially current users. On the other hand, subjects who used non-selective ╬▓-blockers had a higher risk of severe exacerbations in a dose- and duration-dependent manner.
Huang et al. [29] also found betaxolol to be the most effective selective ╬▓-blocker in reducing the risk of severe exacerbations. Betaxolol is considered to be highly cardioselective, and is less likely than other selective ╬▓-blockers to cause pulmonary adverse effects. For non-selective blockers, labetalol and propranolol were found to be significantly associated with an increased risk of severe exacerbations [29]. This may be because labetalol can significantly reduce FEV1 and FVC, while propranolol can reduce FEV1 and the bronchodilator effect of formoterol, thus increasing airway hyperresponsiveness [43].
Another study found the use of carvedilol to be associated with an increased risk of hospitalization for CHF, compared to the use of metoprolol, bisoprolol, and nebivolol [46]. Zvizdic et al. [36] showed that the use of ╬▓-blockers reduced the number of exacerbations over a 12-month period in Global Initiative for Obstructive Lung Disease (GOLD) II individuals. In GOLD III, a severe stage of COPD, the number of exacerbations was not therapy-dependent.
One study has shown that individuals with COPD taking ╬▓-blockers are less symptomatic and have fewer exacerbations, despite receiving fewer respiratory medications. Several factors are related to exacerbations, but only the GOLD stage, use of ╬▓-blockers, use of long-acting beta-agonists (LABA) (including ultra-LABA), and comorbidities had independent effects [25]. In this study, a heart rate greater than 70 bpm was associated with a higher risk of exacerbations, which may indicate that not just ╬▓-blockade, but effective ╬▓-blockade is the likely protective factor. For Puente-Maestu et al. [25], ╬▓-blockers showed a clear protective effect against exacerbations in individuals with COPD.
An overall decrease in long-term bronchodilator use, both long-acting muscarinic antagonists and LABA, was observed. The reasons for this are not clear, but the perception that they can interfere with the ╬▓-blocker, and the non-adherence of patients to various medications [47], may play a role. Interestingly, there is a decrease in the proportion of individuals treated with ŌĆ£traditionalŌĆØ LABAs in the bronchodilator group, which is partly offset by an increase in the use of ultra-LABA. This may show the fear of prescribing ŌĆ£traditionalŌĆØ LABA by physicians who are more aware of the management of heart diseaseŌĆöand also more likely to use ╬▓-blockersŌĆöas there is evidence associating ŌĆ£traditionalŌĆØ LABA with increased mortality in subjects with CHF and CAD [25].
3. Disease severity/severity of illness
Regarding disease severity, Dransfield et al. [19] maintained that cardioselective ╬▓-blockers have no demonstrable effect on lung function, regardless of disease severity or bronchodilator reversibility, and that COPD individuals with heart disease seem to derive the same benefits from these drugs as the general population [48].
Oda et al. [30], which compared the annual changes in lung function in individuals with COPD who took or did not take ╬▓-blockers, it was found that the decline in FEV1 did not differ significantly between the two groups. The use of ╬▓-blockers did not compromise the FEV1 of subjects with COPD. The non-selective ╬▓-blocker used was carvedilol, which, according to the authors, is relatively tolerable in individuals with COPD, promoting mild bronchodilation induced by alpha-adrenergic blockade [49].
Meanwhile, Key et al. [31] showed that ╬▓-blockade had a minimal effect on lung function and dynamic hyperinflation. Bronchodilators, including ╬▓-agonists, are known to produce relatively rapid relaxation of airway smooth muscle and improve expiratory flow rate, but it is questionable whether this is the mechanism by which they act in subjects with COPD, where prominent abnormalities are increased peripheral resistance and the loss of lung elastic recoil [50].
In individuals with COPD, ╬▓-agonists have been shown to reduce inspiratory resistance, but their main effect is to reduce end-expiratory lung volume, which allows the individual to exercise longer, before reaching a critical and limited volume of inspiratory reserve. Therefore, drugs that antagonize airway ╬▓ receptors, and consequently reduce caliber through their effects on smooth muscle, may have little effect on measurements of airway function in individuals with COPD, as this is not predominantly determined by the smooth muscle of the airways [31,51].
Key et al. [31] found that the airway resistance and specific conductance remained unchanged, and ╬▓-blockade did not lead to a significant change in end-expiratory lung volume and magnitude of dynamic hyperinflation during exercise. However, clinical trials have shown that treatment with non-selective ╬▓-blockers in individuals with COPD is associated with a reduction in FEV1, increased airway hyperresponsiveness, and reduced efficacy of bronchodilator treatment [43], which resulted in an increased risk of adverse reactions to pulmonary medications among non-selective ╬▓-blocker users, compared to selective ╬▓-blocker users [46].
Mentz et al. [23] argued that the potential risk of adverse pulmonary effects of non-cardioselective ╬▓-blockers can be balanced by an alternative set of systemic, cardiac, and pulmonary benefits. For example, ╬▓2 adrenergic receptors represent a greater proportion of total cardiac ╬▓ receptors in individuals with CHF, compared to healthy subjects. Individuals with CHF may benefit from antagonism of these receptors by non-selective agents.
Furthermore, non-selective ╬▓-blockers can attenuate the negative effects of ╬▓2 agonists, including dysrhythmogenesis, ischemia, and inflammation [23]. Carvedilol has antioxidant, free radical scavenging, and insulin-sensitizing effects, while ╬▓2 adrenergic receptor antagonism can reduce the release of noradrenaline from myocardial adrenergic nerve terminals, and reduce the complications of hypokalemia [52].
From the perspective of COPD, non-cardioselective ╬▓-blockers can attenuate pulmonary desensitization due to prolonged ╬▓2 adrenergic receptor activation with ╬▓-agonists. ╬▓-Blockers reduce airway hyperresponsiveness, increase pulmonary ╬▓2 receptor regulation, and reduce the need for ╬▓-agonists. ╬▓-Blockers can attenuate the presence of inflammation and reduce mortality and pulmonary exacerbations in subjects with COPD [3,53].
This systematic review and meta-analysis have potential relevance; the protocol for this review was submitted to and registered in the PROSPERO, with the aim of minimizing the risk of publication bias and duplication of reviews that answer the same clinical question. This record also allows us to evaluate the conduct of the study and the quality of reporting its results, increasing transparency and reproducibility.
This study also chose to specifically include a type of study (cohort studies) that allowed better comparison between results; in addition, the authors believe that for the chosen outcomes (disease severity, exacerbations, or mortality) it would be better to include longitudinal studies to evaluate the results over a longer period.
Regarding the limitations of this systematic review and meta-analysis, there was a high rate of heterogeneity between the articles, mainly in relation to the cardiovascular comorbidities studied, and the ╬▓-blockers used. In addition, many studies do not describe the dose prescribed for each ╬▓-blocker, which makes it impossible to compare them adequately.
Another limitation, which is associated with the severity of the disease outcome, was the variability in the ways in which the assessment of lung function was presented in the studies, a factor that also made it impossible to include some articles in the meta-analysis. Due to the form of presentation in each included study, it was also not possible to carry out a meta-analysis evaluating the difference between the diseases.
In conclusion, the use of ╬▓-blockers in individuals with COPD and associated cardiovascular diseases caused positive effects on the mortality and exacerbations outcomes, compared to the results of individuals who did not use them. The severity of the disease caused a slight change in FEV1. These data contribute to greater safety in the use of ╬▓-blockers in this population profile. However, there was high heterogeneity between the studies, especially in relation to cardiovascular comorbidities and the ╬▓-blocker used. As a result, further studies are needed: both observational cohort and clinical trials that aim to study the effect of using a specific ╬▓-blocker in COPD associated with a specific cardiovascular comorbidity.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






