



Introduction
Clonal hematopoiesis of indeterminate potential (CHIP) is a phenomenon in which somatic mutations in hematopoietic stem cells result in the clonal outgrowth of a mutant population of blood cells in individuals without hematologic malignancy [1]. The prevalence of CHIP is known to increase with age, and it is rarely found in patients <40 years but in >5% of patients in their 60s [2]. Based on the results of basic and animal studies of genetic mutations in CHIP, CHIP induces chronic inflammation through inflammasome activation in innate immune cells and, consequently, may contribute to the development of various chronic diseases [3]. Recent studies have reported that CHIP is associated with an increased risk of hematological malignancy and cardiovascular disease [4], even with infection control [5].
Chronic obstructive pulmonary disease (COPD) is characterized by persistent and progressive airflow limitation, and is a significant cause of long-term morbidity and mortality [6]. A key mechanism underlying the development of COPD is chronic neutrophilic inflammation associated with the repetitive inhalation of toxic particles, which is associated with a decline in lung function and risk of acute exacerbation in patients with COPD [7,8]. Neutrophilic inflammation and the associated cytokine cascades are among the major mechanisms of CHIP, indicating that CHIP may serve as a biomarker for the development and progression of COPD [9].
In fact, a recent study showed a higher prevalence of CHIP in COPD patients compared to non-COPD patients, suggesting that CHIP may be a biomarker for the development of COPD [10]. However, whether CHIP can be a biomarker for phenotyping COPD, including smoking status, severity of airflow obstruction and exacerbations, has not been clarified. Therefore, we aimed to evaluate the association between CHIP and disease characteristics focusing on smoking status and disease severity in COPD patients.
Materials and Methods
1. Study design and participants
Eligible participants were patients who underwent pulmonary function tests and were diagnosed with COPD based on the following spirometric criteria: post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio of <0.7. Patients with active hematologic malignancy were excluded from this study. The participants were enrolled from the Seoul National University Hospital Airway Registry (NCT02527486) from January 2013 to December 2019, and blood samples were acquired at the time of registry enrollment. Written informed consent was obtained from all participants. This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. H-2012-127-1183).
Symptoms were estimated using the COPD assessment test (CAT) score, St. GeorgeŌĆÖs Respiratory Questionnaire (SGRQ) score, and modified Medical Research Council (mMRC) grade. According to the recent Global Initiative for Obstructive Disease (GOLD) guidelines, the severity of airflow obstruction was classified based on spirometric measurements, as follows: GOLD grade 1, FEV1 Ōēź80% predicted; GOLD grade 2, 50%Ōēż FEV1 <80% predicted; GOLD grade 3, 30%Ōēż FEV1 <50% predicted; GOLD grade 4, FEV1 <30% predicted [11]. Additionally, we re-classified GOLD grade 1 as mild COPD, grade 2 as moderate COPD, and grades 3-4 as severe COPD for further analysis. History of acute exacerbation in the past year was reviewed as another clinical outcome. Acute exacerbation of COPD was defined as the acute worsening of respiratory symptoms that resulted in additional treatment and was classified as mild (treated with short-acting bronchodilators only), moderate (treated with oral antibiotics and/or oral corticosteroids), or severe (requiring emergency room visits or hospitalization) [12]. Frequent exacerbation was defined as having Ōēź2 moderate exacerbations or Ōēź1 severe exacerbations during the previous year. All participants were assessed for self-reported smoking status (current smoker, ex-smoker, and never-smoker) and smoking intensity (pack-year).
2. Assessment of CHIP
Targeted gene sequencing was performed on 2├Ś100 bp paired-end reads over a minimum coverage of 1,000x (median coverage 2,225x; 1,109x-4,317x). This analysis focused on mutations in 25 immune-related genes related to CHIP. Using IlluminaŌĆÖs bcl2fastq (v2.17.1.14, Illumina, San Diego, CA, USA), we demultiplexed targeted sequencing data for peripheral blood mononuclear cell samples to produce FASTQ files. We calculated duplication metrics and binary alignment map (BAM) quality metrics with PICARD (v1.94, Github, San Francisco, CA, USA). The BAM files prepared for analysis underwent a somatic variant calling process that included VarDict [13], Mutect2 (4.1.4.1) [14], and SNVer (0.4.1) [15] for identifying single nucleotide variants, insertions, and deletions. We screened out a subset of potential false positives with a minor allele frequency exceeding 1.5% in somatic variants, based on negative cohort data that arenŌĆÖt present in Catalogue of Somatic Mutations in Cancer (COSMIC) hematological criteria. Afterward, a review using Integrative Genomics Viewer was conducted to exclude variants likely caused by polymerase chain reaction artifacts, highly similar sequences, and repetitive regions. We considered a variant allele fraction of 1.5% or higher as significant for genetic mutations and used this as the criterion for CHIP status.
3. Study outcomes
We evaluated the prevalence of CHIP in patients with COPD. This prevalence was based on smoking status, which was classified as current and non-current (never- and ex-smoker), and severity of airflow obstruction, which was classified as mild (GOLD grade 1) or moderate-to-severe (GOLD grade 2-4) [11]. The primary outcome was the association between the CHIP score, smoking status, and severity of airflow obstruction. The secondary outcome was the association between CHIP score, lung function, symptoms and acute exacerbation. FEV1 and the FEV1/FVC ratio were selected as lung function indices in this study based on their established association with COPD progression [16].
4. Statistical analysis
Continuous variables are presented as mean and standard deviation, and categorical variables are presented as numbers and percentages. The chi-square test, FisherŌĆÖs exact test, and t-test were used to compare the baseline characteristics of the study population between the groups. Logistic regression analyses were performed to evaluate the association of CHIP with smoking status and COPD severity. Multivariable analysis was adjusted for age, sex, FEV1, and smoking status/intensity. Linear regression and Poisson regression analysis were performed to examine the association of CHIP with lung function and the frequency of acute exacerbation, respectively. Odds ratios (ORs) and adjusted ORs (aORs) are reported together with 95% confidence intervals (CI). Results with two-tailed p-values <0.05 were considered statistically significant. Statistical analyses were conducted using the SPSS software version 26.0 (IBM Corp., Armonk, NY, USA).
5. Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request. The corresponding author has full access to all data used in this study and has the final responsibility for the decision to submit the manuscript for publication.
Results
1. Baseline characteristics of the study population
A total of 125 COPD patients were included in the primary analysis; the mean age was 68.1 years, and proportion of male patients was 89.6%. Table 1 presents the baseline characteristics of the study population. While the current smoker group had 34 patients (27.2%), the non-current smoker group had 91 patients (72.8%), with 21 never-smokers and 70 ex-smokers. There were no significant differences in baseline characteristics, including smoking intensity, between the current and non-current smoker groups. While the study population was additionally classified into never-smokers, ex-smokers, and current smokers, never-smoker group had significantly higher proportion of female sex, higher FEV1 % predicted and FEV1/FVC ratio, compared to other groups (Supplementary Table S1).
When classifying the study population by severity of airflow obstruction, 16 patients (12.8%) had GOLD grade 1 and 109 patients (87.2%) had GOLD grade 2-4. The GOLD grade 2-4 group had significantly lower FEV1, FVC, and FEV1/FVC ratios than the GOLD 1 group. Smoking intensity, symptom status, quality of life, 6-minute walking distance, and exacerbation frequency were not significantly different between GOLD 1 and GOLD 2-4 groups. When classifying COPD patients according to the severity of airflow limitation as mild, moderate, and severe, we observed a significant and gradual decrease in FEV1, FVC, and FEV1/FVC ratio from mild to moderate and then severe COPD (Supplementary Table S2). Similarly, in this classification, there was no significant difference in the history of acute exacerbations from the previous year among the groups.
2. Association between CHIP and smoking status
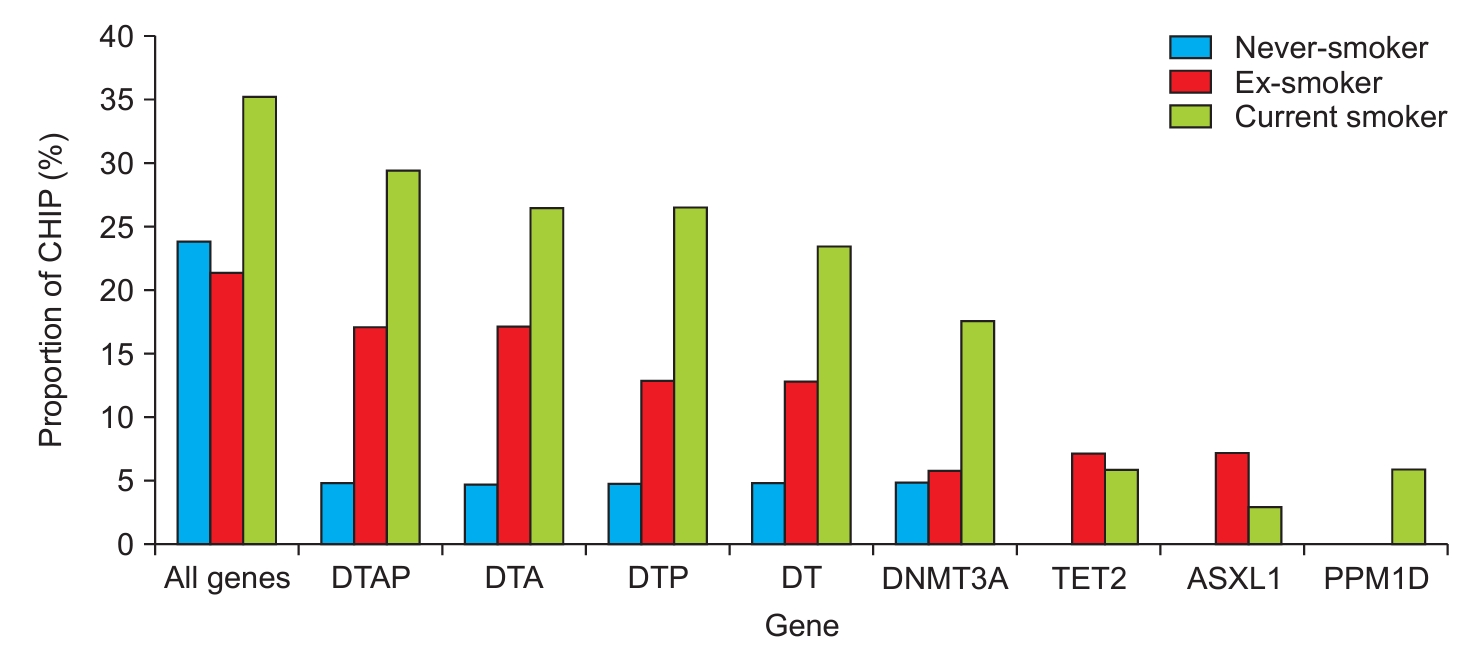
We identified CHIP in 32 (25.6%) study participants. Although the differences in baseline characteristics based on CHIP status were not statistically significant, the CHIP-positive group exhibited a tendency towards a higher proportion of current smokers and a higher smoking intensity compared to the CHIP-negative group (Supplementary Table S3). Figure 1 presents the distribution of CHIP scores according to smoking status. In the analysis of all genes, CHIP was identified in 23.8% of never-smokers, 21.4% of ex-smokers, and 35.3% of current smokers. The five most commonly identified CHIPs were mutations in the combination of DNMT3A, TET2, ASXL1, and PPM1D (DTAP), combination of DNMT3A, TET2, and ASXL1 (DTA), combination of DNMT3A, TET2, and PPM1D (DTP), and combination of DNMT3A and TET2 (DT) genes, and the prevalence of these genes was observed highest in current smokers, followed ex-smokers, and never-smokers in that order. When categorizing smoking status into current and non-current smokers for analysis, there was a tendency for higher CHIP prevalence in current smokers across most genes, with a significantly higher prevalence of CHIP observed in the DTP, DNA methyltransferase 3 alpha (DNMT3A), and protein phosphatase, Mg2+/Mn2+ dependent 1D (PPM1D) genes than in non-current smokers (Table 2). When classified into never-smokers, ex-smokers, and current smokers based on smoking history, no significant differences in CHIP prevalence were observed according to smoking status (Supplementary Table S4).
In the analysis of all investigated genes, CHIP showed no significant association with current smoking (Table 3). However, CHIP in the DTP and DNMT3A genes were significantly associated with current smoking in the univariable analysis (OR, 2.92; 95% CI, 1.07 to 7.97; p=0.037) (OR, 3.69; 95% CI, 1.04 to 13.0; p=0.043). These associations were consistent in the multivariable analysis (aOR, 2.80; 95% CI, 1.01 to 7.79; p=0.048) (aOR, 4.03; 95% CI, 1.09 to 14.0; p=0.037).
3. Association between CHIP and severity of airflow obstruction
The severity of airflow obstruction was analyzed by categorizing it into mild (GOLD 1) and moderate-to-severe grade (GOLD 2-4) (Table 2). The results showed that in the GOLD 2-4 group, there was a tendency for a higher prevalence of CHIP in almost all genes compared to that in the GOLD 1 group, but this was not statistically significant. The prevalence of CHIP, when classified based on the severity of airflow obstruction into mild, moderate, and severe, similarly did not show a significant association with the severity of airway obstruction (Supplementary Table S5). In addition, in both the overall and individual genes, CHIP showed no significant association with the GOLD groups (Table 4).
4. Association of CHIP with acute exacerbation, lung function, and symptoms
We analyzed the association among CHIP, acute exacerbation history in the past year, lung function, and symptom burden. The analysis of acute exacerbation revealed that CHIP in ASXL transcriptional regulator 1 (ASXL1) genes was significantly associated with history of mild, severe, and total acute exacerbation (Table 5). While additional analysis was conducted to evaluate the association between CHIP and acute exacerbation of COPD according to severity of exacerbation, CHIP in DTA and ASXL1 genes were positively associated with a higher number of severe acute exacerbation history in the past year (╬▓┬▒standard error [SE] 1.16┬▒0.54, p=0.032; ╬▓┬▒SE 2.23┬▒0.59, p<0.001). There was no significant association between frequent exacerbation and CHIP.
CHIP in both the overall and individual genes was not associated with FEV1 or FVC or the FEV1/FVC ratio (Supplementary Table S6). And, there was no CHIP gene significantly associated with SGRQ score, CAT scores, and mMRC grade (Supplementary Table S7).
Discussion
This study demonstrated that the prevalence of CHIP in patients with COPD is the highest in current smokers, followed by ex-smokers and never-smokers. Smoking is a risk factor for the development of CHIP and is associated with the risk of smoking-related diseases [17]. Mutations in somatic cells related to CHIP are found in a limited number of genes, most of which are associated with DNA methylation and regulate the epigenome function of the epigenome [2,18]. Smoking has a causal association with mosaic chromosomal alterations [19], and if the function of these genes is impaired by smoking-induced mutations, this can lead to the subsequent accumulation of other genetic mutations [1]. This process may result in increased CHIP associated with smoking, which could serve as a precursor for the progression of smoking-related diseases such as COPD.
Our major findings indicated that CHIP in the DTP and DNMT3A genes was significantly associated with current smokers compared to non-current smokers in both univariable and multivariable analyses. This is consistent with the findings of the UK Biobank cohort study based on genome-wide association analysis, which showed a significant association between CHIP of specific genes and current smoking, compared with past smoking [20]. This finding suggests that the active inflammatory microenvironment induced by current smoking influences the occurrence and maintenance of somatic mutations. A study conducted on smokers in the COPDGene cohort showed that current smoking is a significant predictor of COPD progression [16]. Furthermore, in the Copenhagen General Population Study, current smoking in patients with COPD was associated with a significantly higher risk of hospitalization due to COPD, pneumonia, and all-cause mortality compared to ex- and never-smokers [21]. We could postulate that some of these smoking-related poor outcomes are mediated by CHIP. CHIP in COPD patients may serve not only as an indicator of the current inflammatory condition related to smoking status but also as a potential prognostic biomarker for future outcomes.
In this study, the prevalence of CHIP tended to be higher in moderate-to-severe COPD than in mild COPD, although the difference was not statistically significant, and there was no significant association between moderate-to-severe COPD and CHIP. This may be partly due to a low statistical power by the small number of study participants at each spirometric measurements of COPD, which could have limited the statistical power. A recent study from the COPDGene cohort reported that CHIP, as identified through whole-genome and whole-exome sequencing, was associated with a 1.6-fold higher risk of moderate-to-severe COPD [10]. In a mouse model of cigarette smoke exposure, functional loss related to CHIP of the tet methylcytosine dioxygenase 2 (TET2) gene resulted in pulmonary inflammation, increased interferon signaling, and aggravation of emphysema, leading to the development of COPD. Considering previous research findings, our study suggests that the higher prevalence of CHIP in more severe COPD, as observed in our study, may be associated with CHIP-induced aberrant immune cell function, potentially augmenting inflammatory stimuli and worsening COPD.
Given the association between lung function and CHIP, COPDGene cohort study demonstrated that CHIP was associated with decreased FEV1 % predicted in COPD GOLD 2-4 [10]. Another study analyzing CHIP with deep-targeted amplicon sequencing from COPD patients confirmed that CHIP mutations with a predominance of the DNMT3A gene and CHIP-mediated hypomethylation of phospholipase D family member 5 are positively correlated with increased levels of pro-inflammatory cytokines and decline of lung function [22]. We analyzed FEV1 and FEV1/FVC ratio, which are representative indicators of COPD severity and obstructive ventilatory disorder, respectively. In contrast to previous studies, we found no significant association between CHIP levels and these two lung function indicators. The statistical significance in our study was not the current disease state (COPD severity) but rather the current inflammatory environment (current smoking status). This suggests that CHIP may be more closely related to future changes in lung function due to current inflammation, rather than the current lung function itself. Further research is required to explore whether longitudinal changes in lung function are associated with CHIP.
In the analysis of exacerbation history, CHIP was significantly associated with acute COPD exacerbation in the past year. In patients with COPD, acute exacerbation augments the decline in lung function and is associated with disease progression, which is a strong risk factor for future exacerbation [23,24]. While this study did not determine the association between CHIP and long-term clinical outcomes of COPD, the results suggest the potential value of CHIP as a predictive indicator of disease status and future course.
This study had several limitations. First, the small sample size limited the statistical power of the study results and the availability of additional subgroup analyses. Second, the genetic changes associated with smoking exposure and COPD progression may vary by ethnicity; however, this study included only an Asian population, which limits its generalizability. Third, we determined smoking status based on the participantsŌĆÖ smoking history at the time of enrollment in the study. It is possible that there were changes in the smoking status of the participants during the study period; however, these changes were not considered in the analysis. Fourth, this study did not include laboratory and radiological data, therefore, an analysis of the association of CHIP with the severity of inflammatory markers and imaging findings was not available.
In conclusion, in patients with COPD, CHIP in specific genes was significantly associated with current smoking status, compared to never- and ex-smokers, and with a higher number of acute exacerbation history in the past year.
Given that both a current smoking status and a history of acute exacerbation in the past year are predictive of poor outcomes, CHIP may be not only an indicator of current smoking-related inflammation but also a potential prognostic biomarker for future outcomes. Further studies are needed to evaluate the clinical significance of CHIP as a biomarker in the long-term course of COPD.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Supplement1
Supplement1 Print
Print Download Citation
Download Citation






