


Introduction
Primary tracheal amyloidosis (PTA) is a very rare form of amyloidosis. The most common presenting symptom is dyspnea caused by deposition of insoluble protein fibrils in the central airway walls1,2. This severe disease can develop respiratory failure requiring aggressive intervention, including intubation and mechanical ventilation, to maintain airway patency.
Bronchoscopic intervention restores airway patency in patients with benign airway obstruction, such as post-intubation and post-tuberculosis stenosis3,4. Several reports have described the outcomes from bronchoscopic intervention in patients with PTA5,6. However, scant information regarding the usefulness of silicone stent placement in patients with PTA is available. Herein, we report a case of diffuse PTA with tracheomalacia causing severe cartilage destruction that was managed successfully by bronchoscopic intervention and the placement of a silicone stent.
Case Report
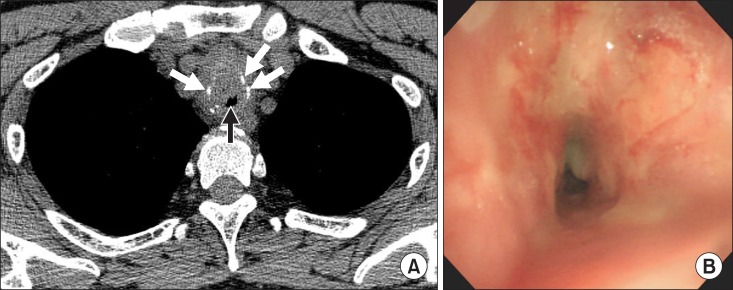
A 48-year-old male presented to the emergency department with respiratory distress. He complained of progressive dyspnea of 2 weeks' duration, and endotracheal intubation was performed due to impending respiratory failure. A chest computed tomography scan revealed luminal narrowing, irregular wall thickening, and severe cartilage destruction in the trachea (Figure 1A).
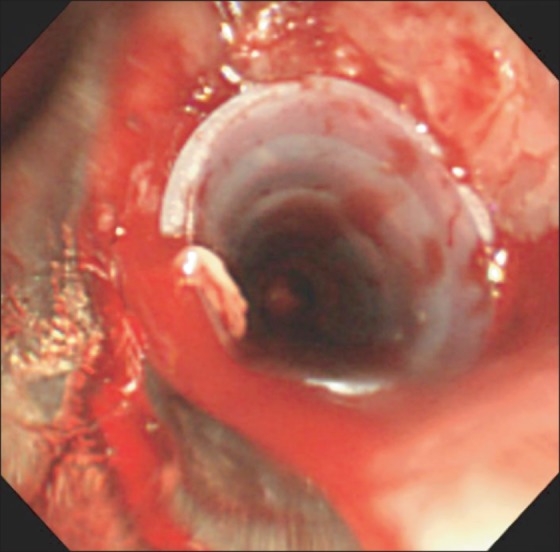
To evaluate the tracheobronchial tree and restore airway patency, rigid bronchoscopy was performed. Initial bronchoscopic findings showed circumferential airway narrowing with exudate (Figure 1B). Ballooning (Boston Scientific, Natick, MA, USA) was performed to mechanically dilate the narrowed airway, and a large amorphous mass was resected by bougienation using the bevel of the rigid bronchoscope (Karl-Storz, Tuttlingen, Germany). After airway dilatation, severe tracheomalacia, causing cartilage destruction and fragmentation, was noted. A silicone airway stent (TNO, Seoul, Korea) was placed to maintain airway patency (Figure 2).
The pathological samples obtained from the tracheal lesions showed fibrosis and amorphous eosinophilic material that selectively stained with Congo Red. Thus, a diagnosis of tracheobronchial amyloidosis was confirmed (Figure 3). The patient experienced symptomatic improvement immediately following rigid bronchoscopy with stenting and was discharged 3 days after the intervention. There were no respiratory symptoms or procedure-related complications during the 6-month follow-up period. A normal pulmonary function test was reported 6 months following bronchoscopic intervention.
Discussion
Although amyloidosis rarely involves the respiratory tract, life-threatening airway obstruction can develop in patients with severe PTA7. To prevent respiratory arrest and maintain airway patency, bronchoscopic intervention using a rigid bronchoscope is essential. Focal airway involvement can be treated with mechanical dilatation using laser cauterization, ballooning, or bougienage6. However, complex PTA with diffuse airway involvement and concomitant cartilage destruction leads to the loss of airway wall structural integrity. In these cases, airway stent implantation should follow mechanical dilatation.
Recently, a self-expanding metal stent was reported as a possible treatment for severe PTA8. However, metallic stents exert a significant radial force on the tracheal wall and integrate into the airway. This may lead to stent-related complications such as granulation tissue overgrowth, stent fracture, and erosion into the great vessels or the esophagus9,10. The United States Food and Drug Administration has issued a warning for metallic stents in the treatment of benign airway disease due to these complications10. Silicone stents are a reasonable treatment option when an airway stent is indicated for PTA.
The patient had PTA with destruction and fragmentation of the tracheal cartilage. Therefore, mechanical dilatation alone was insufficient to maintain tracheal lumen patency. A silicone stent was placed; this stabilized the patient. Pulmonary function tests remained normal during the 6-month follow-up period. This case demonstrates that silicone airway stenting is a useful and safe therapeutic strategy for patients with severe PTA and intractable airway malacia.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






