



Introduction
Sepsis is a life-threatening condition accompanied by organ dysfunction caused by a dysregulated host response to infection [1]. Mortality rate ranges from 10% in patients with sepsis to more than 40% in patients with septic shock. Acute respiratory distress syndrome (ARDS) is a fatal condition that commonly develops in patients with sepsis. ARDS is not uncommon reason for intensive care unit (ICU) admission and require invasive mechanical ventilation (IMV) [2]. The mortality rate of ARDS still remains high despite of advances in critical care medicine and research [2,3]. The key pathogenetic mechanism of ARDS is the complex inflammatory response [4], which results in hypoxemia and abrogation of aerobic metabolism. Adjunct pharmacological therapies in patients with ARDS have been tried, but their clinical benefit is yet to be proven robustly [5-7].
Vitamin B1 is involved in aerobic metabolism [8], and vitamin C has anti-inflammatory and anti-oxidative effects [9,10]. Vitamin B1 and C deficiencies have been reported in critically ill patients with sepsis [11,12]. Two retrospective studies have reported that intravenous administration of vitamin B1 or C improves clinical outcomes in critically ill patients with septic shock or severe pneumonia [13,14]. However, recent studies did not show the clinical benefits of the combination of vitamin B1, C, and hydrocortisone [15,16]. The clinical implication of intravenous administration of vitamin B and C on patients with sepsis-related ARDS was not elucidated.
The aim of this study was to evaluate the clinical impact of vitamin B and C supplementation in patients with sepsis-related ARDS.
Materials and Methods
1. Patients
From June 2017 to May 2019, the clinical data of patients older than 18 year olds with sepsis-related ARDS who received IMV and admitted at the 13-bed medical ICU (MICU) of the tertiary hospital were retrospectively reviewed. All patients under IMV met the Berlin criteria for ARDS [17]. Since June 2018, vitamin B1 and C supplementation was initiated in MICU. Patients at 1-year before vitamin B1 and C supplementation were designated to the control group, whereas those at 1-year after vitamin B1 and C supplementation was to the supplementation group. The characteristics and clinical outcomes were compared between the two groups.
The total supplementation of vitamin B1 was 200 mg/day as recommended by the guideline [18]. Vitamin B1 was intravenously infused 50 mg every 6 hours. The optimal dose of vitamin C has not been established, although several studies have reported that high dose vitamin C administration was effective in critically ill patients. Presently, we gave intravenously administered a total 2 g of vitamin C in accordance with a recent pharmacokinetic study which showed that at least 2 g of vitamin C was sufficient to maintain vitamin C concentration in the blood of critically ill patients [19]. Vitamin C was intravenously infused 500 mg every 6 hours. Vitamin B1 and C was given intravenously until death at MICU, reversal of shock, until MV weaning or discharge at MICU.
2. Data collection
Baseline (age, sex, body mass index, comorbidities) and clinical characteristics (presence of shock, acute kidney injury, and management) were assessed. The severities of illness Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Sequential Organ Failure Assessment (SOFA) score were noted. Additionally, the data of various laboratory parameters (white cell count, hemoglobin, platelet, C-reactive protein, albumin, procalcitonin, partial pressure of carbon dioxide, and partial pressure of oxygen/fractionated inspired oxygen) were collected. Moreover, clinical outcomes (ventilator-free and ICU-free day at 30 days, mortality) were analyzed.
This study was approved by the Institutional Review Board of Gyeongsang National University Hospital (IRB No. 2019-03-001). The requirement of informed consent was waived because of the retrospective nature of the study. The study was conducted in accordance with the ethical standards of institutional and/or national research committees and adhered to the tenets of the Declaration of Helsinki and its later amendments or comparable ethical standards.
3. Statistical analysis
Categorical variable are expressed as and compared with chi-square or Fisher’s exact tests. Continuous variables are presented as median and interquartile range or as mean±standard deviation, unless indicated otherwise, and compared with Mann-Whitney U or Student’s t-tests. Factors associated with mortality were evaluated with Cox proportional hazards regression analysis. Propensity score matching method was performed to consider for the differences in baseline and clinical characteristics. Matched variables were age, gender, APACHE II score, SOFA score, use of neuromuscular blocking (NM) blockers, steroid, and prone position. Based on the standard deviation of the logit of the estimated propensity score, 1:1 matching was performed using the nearest-neighbor method with a caliper width of 0.2 in a pairwise manner. All tests of significance were two-tailed. A p-value of 0.05 was considered statistically significant. All data were analyzed with SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
1. The characteristics of the patients
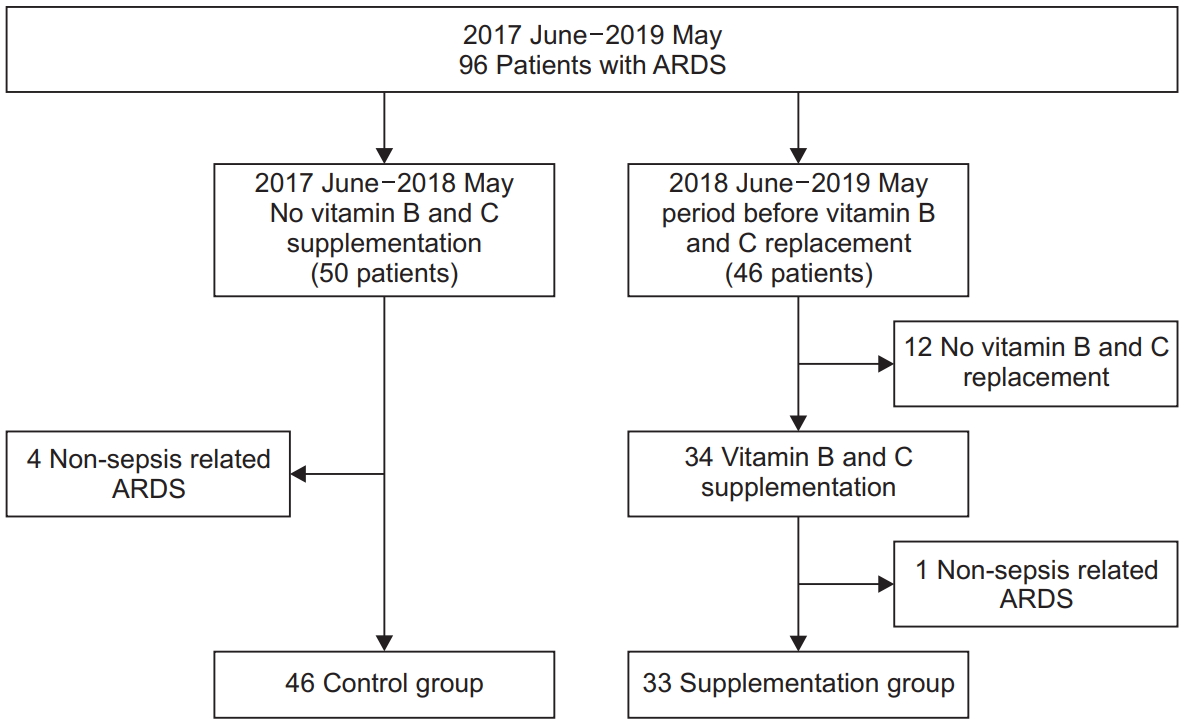
During the 2-year study period, 96 patients with ARDS were admitted to the MICU (Figure 1). From June 2017 to May 2018, before vitamin B1 and C supplementation, 50 patients were admitted because of ARDS and sepsis-related ARDS was in 46 patients (control group). From June 2018 to May 2019, 46 patients with ARDS were admitted to MICU and 34 patients (73.9%) of them received vitamin B1 and C supplementation (supplementation group) with exception of one patient, 33 patients were diagnosed with sepsis-related ARDS. The characteristics were compared between the control (n=46) and supplementation (n=33) groups and the data are shown in Table 1. Median duration of vitamin B1 and C was 6 days and interquartile range was 3.5-10 days.
The median age of patients was 70 years old and 70% among them were men. There was no significant difference in the baseline characteristics, and severity of illness scores. In mechanical ventilator parameters, there was no significant difference in two groups. The NM agents were more used in vitamin B1 and C supplementation group than in control group.
Steroid administration and prone positioning of patients were significantly frequent in the supplementation group than those in control group. There were no significant differences in the proportion of patients who had acute kidney injury and or those who underwent renal replacement therapy or extracorporeal membrane oxygen therapy.
The values of laboratory parameters and severity of ARDS were compared and are shown in Table 2. Regarding the values of laboratory parameters, no significant differences were observed between the two groups. There was a higher trend toward severe ARDS in the supplementation group than control group (57.6% vs. 37%, p=0.095).
2. Clinical outcomes and factors associated with 30-day mortality
The clinical outcomes are shown in Table 3. There were no significant differences in the rates of mortality between two groups. Both mean ventilator-free and ICU-free days at day 30 were significantly longer in the supplementation group than that in the control group (7.7±10.8 days vs. 2.7±7.3 days, p=0.014 and 6.9±9.8 days vs. 2.2±6.5 days, p=0.009).
The factors associated with 30-day mortality were evaluated using Cox proportional hazards regression analysis and are shown in Table 4. On univariate and multivariate analyses, APACHE II score was associated with 30-day mortality (hazard ratio [HR], 1.073; confidence interval [CI], 1.025-1.122; p=0.002). Supplementation of vitamin B1 and C showed no association with 30-day mortality.
Propensity score matching yield 21 pairs of supplemented and control patients who had similar characteristics including age, sex, APACHE II score, SOFA score, use of NM blockers, steroid, and prone position. In matched patients, there were no significant differences in 30-day morality between supplementation and control group (57.1% vs. 66.7%, p=0.525). Both mean ventilator-free and ICU-free days at day 30 were a longer trend toward supplementation group than control group, respectively (7.3±11 days vs. 2.4±7.7 days, p=0.079 and 6.9±9.8 vs. 2.2±6.5, p=0.096). Propensity matched analysis also showed that supplementation of vitamin B1 and C was not associated with 30-day mortality (HR, 0.808; 95% CI, 0.377-1.730; p=0.808).
Discussion
In the current study, supplementation of vitamin B1 (200 mg/day) and vitamin C (2 g/day) showed no improvement in the mortality of patients with sepsis-related ARDS. The mean ventilator-free and ICU-free days at day 30 were longer in patients supplemented with vitamin B1 and C than that in the control patients but in matched group, there were no significant different. APACHE II score was associated with the 30-day mortality; however, supplementation with vitamin B1 and C showed no effect on 30-day mortality.
Sepsis is a common condition for ICU admission and accounts for a substantial mortality rate in critically ill patients [1]. ARDS is one of the life-threatening organ dysfunctions in sepsis [20]. The prevalence of ARDS was about 10% of all ICU admissions and mortality rate was high up to 40% in severe case [2]. Systemic inflammation is one of the pathogenetic mechanisms in sepsis-related ARDS [21,22]. Inflammation also plays a role in the generation of oxidative stress. Severe lung injury due to inflammation causes hypoxemia, which eventually causes the dysfunction of aerobic metabolism. Mitigation of inflammatory and oxidative stress and facilitation of aerobic metabolism are presumably important to improve the clinical outcomes in patients with sepsis-related ARDS. Protective mechanical ventilation has been advanced to improve the clinical outcome in patients with ARDS. However, clinical trials assessing the efficacy of adjunct pharmacotherapy showed no consistent association with reduced mortality rate of patients with ARDS [5-7].
Vitamin C is hydrophilic and excreted in urine and has multiple effects such as anti-inflammation, anti-oxidation, etc. [23]. Vitamin C is a cofactor for an enzyme which activates the endogeneous catecholamine production pathway [24]. Vitamin B1 (thiamine) is a water-soluble and crucial vitamin for aerobic metabolism. It is a cofactor for pyruvate dehydrogenase, which converts pyruvate into acetyl-coenzyme A to enter the tricarboxylic acid cycle [8]. Moreover, vitamin B1 reduces oxalate excretion by acting as coenzyme in vitamin C metabolism [23].
Some studies have reported that low vitamin C level in critically ill patients [12]. Vitamin C deficiency is associated with coagulation abnormalities, and endothelial dysfunction [25]. Vitamin B1 deficiency has been reported approximately up to 70% of critically ill patients and may be associated with increased mortality [26]. One study reported that thiamine supplementation was associated with lower creatinine levels and a lower rate of progression on renal replacement therapy in patients with septic shock [27]. Another study reported that early thiamine administration in patients with septic shock is associated with reduced 28-day mortality [28].
Two retrospective studies (one on septic shock and the other on severe pneumonia) reported that combined administration of vitamin B1, C, and hydrocortisone was associated with improved clinical outcomes [13,14]. However, two recent studies demonstrated no such clinical benefits of early vitamin C and thiamine administration in patients with septic shock in emergency department [15,16]. Vitamin C monotherapy was ineffective to improve clinical outcome in patients with severe sepsis or septic shock receiving mechanical ventilation [29]. The clinical implication of combined vitamin B1 and C administration and the optimal dose remains undefined. The clinical data of vitamin B1 and C supplementation on patients with sepsisrelated ARDS are still lacking. The present study evaluated the clinical benefit of vitamin B1 and C supplementation in patients with sepsis-related ARDS. There were no significant differences in mortalities between the supplementation and control groups. The ventilator-free and ICU-free days at day 30 were significantly longer in supplementation group than those in the control group. However, there was no significant different in 21 matched patients using propensity score matching method. Patients in control group were older and had more the proportion of comorbid diseases than those in supplementation group. This might affect the ventilator-free day and ICU-free day in unmatched groups. On multivariate analyses, the severity of illness was associated with 30-day mortality, but not with vitamin B1 and C supplementation. The current study showed no improvement in the mortality of patients with ARDS in the supplementation group, which contradicts the results of previous retrospective studies. The following reasons may explain the incongruence of results. First, different characteristics of patients may be different among the studies. Second, the dose of vitamin B1 and C administered was lower than that administered in the previous studies. The current guideline did not support the administration of high doses vitamin, although the administration of high dose vitamin C (≥3 g/day) was associated with reduced mortality rate in some studies. Third, all patients assessed in this study did not receive steroid administration whereas most of patients in the two previous studies received steroid administration. Although, theoretically, the combined use of corticosteroid and vitamin C has a synergistic effect, the current sepsis guideline does not recommend corticosteroid administration except in case of refractory hypotension. The clinical benefit of steroid administration in patients with ARDS is still controversial. Steroid was used in patients with refractory septic shock, exacerbation of existing airways disease. The use of steroid in ARDS was determined by the attending physician.
The current study has several limitations. The first, because of the single center, retrospective study design, selection bias cannot be excluded. The second, some patient did not receive vitamin B1 and C administration during supplementation period, which limits the general interpretation of clinical outcomes of the present study. The third, we did not supplement high dose vitamin B1 and C as previous studies. The optimal dose of vitamin B1 and C supplementation was not defined, and moreover, the current guidelines does not recommend administration of high doses of vitamin B1 and C. The fourth, the biological levels of vitamin B1 and C were not measured. Patients with low vitamin B1 and C levels might, therefore, have more clinical benefits than those with sufficient serum vitamin B1 and C levels. The fifth, all patients in the vitamin B1 and C supplementation group did not get steroids.
In conclusion, vitamin B1 (200 mg/day) and C (2 g/day) supplementation in patients with sepsis-related ARDS requiring invasive mechanical ventilation was not associated with reduced mortality rates, ventilator and ICU-free days. This finding suggests 2 g/day of vitamin C is inadequate to show survival benefit in patients with sepsis-related ARDS. Large prospective randomized controlled studies will be needed to conclusively verify the clinical benefit of vitamin B1 and C supplementation in patients with sepsis-related ARDS.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






