Efficacy of Induced Sputum for the Diagnosis of Pulmonary Tuberculosis in Adults Unable to Expectorate Sputum
Article information
Abstract
Background
Induced sputum (IS) has been used to collect airway secretions in subjects who have inadequate sputum production. The aim of this study was to investigate the efficacy of IS for the diagnosis of pulmonary tuberculosis (PTB) in adults unable to expectorate sputum.
Methods
Medical records of 39 PTB patients who underwent IS due to absence of spontaneous sputum production between January 2011 and March 2014 at a tertiary hospital in South Korea were reviewed. Results of acid fast bacilli smear, Mycobacterium tuberculosis culture and polymerase chain reaction assay for M. tuberculosis (TB-PCR) of IS specimens from these patients were analyzed. Clinical and high-resolution computed tomography (HRCT) characteristics were also analyzed to find characteristics associated with IS culture positivity.
Results
Of the 39 IS specimens from PTB patients, 7 (17.9%) were smear positive and 31 (79.5%) were culture positive. Twenty-four IS specimens were tested for TB-PCR and 13 (54.2%) were positive on TB-PCR. Multivariate analysis showed that younger age (p=0.04) and presence of tree-in-bud appearance on HRCT (p=0.03) were independent predictors of IS culture positivity.
Conclusion
IS is useful for the diagnosis of PTB in adults unable to expectorate sputum. Younger age and tree-in-bud appearance on HRCT were associated with IS culture positivity in these patients.
Introduction
Sputum acid-fast bacilli (AFB) smear and culture for Mycobacterium tuberculosis have been the gold standards for the diagnosis of pulmonary tuberculosis (PTB). However, some patients with radiological suspicion of PTB are unable to expectorate sputum1. Thus, an alternative method of obtaining sputum specimens is needed in these patients.
Hypertonic saline inhalation irritates the airways causing the patient to cough and increases mucus production by the submucosal glands2. Induced sputum (IS) has been advocated as a useful tool to obtain respiratory specimens in PTB suspects who are spontaneous sputum smear negative or unable to expectorate sputum3. Anderson et al.3 compared IS and bronchoscopy in the diagnosis of smear negative PTB, and reported that the diagnostic yield of IS was equivalent to that of bronchoscopy. Similar results were obtained from a larger study in Brazil4. IS also have several advantages over bronchoscopy, which include less invasiveness, greater patient comfort and safety, low-cost and no need for expert for performance3. Thus, IS has been proposed to be used before bronchoscopy to obtain airway secretion from PTB suspects who are unable to expectorate sputum35. However, a few studies in developed countries showed that efficacy of IS is limited for the diagnosis of smear negative PTB and suggested that early bronchoscopy referral may be the preferred diagnostic modality over IS67.
Diagnosis of PTB is often delayed because the sensitivity of AFB smear is poor and culture for M. tuberculosis, which is more sensitive than AFB smear, requires several weeks to get results. The delay in diagnosis of PTB is a serious problem in clinical practice because delayed treatment causes spread of infection and increases the severity of the disease. Empirical treatments of PTB have been tried if presumptive diagnosis of PTB is possible based on clinical and radiological findings8.
The clinical characteristics of PTB patients have limited value for the diagnosis of PTB9. Clinical characteristics of PTB in patients who are unable to expectorate sputum have not been described previously. Recently, high-resolution computed tomography (HRCT) has been shown to be superior to chest X-ray in the diagnosis of PTB because it provides more accurate information about the characteristic findings of PTB10. In one study conducted among smear negative PTB suspects, the sensitivity and specificity of HRCT in the diagnosis of PTB was 88% and 88%, respectively11. However, HRCT findings has not been thoroughly validated in PTB patients who are unable to expectorate sputum.
This study assessed the utility of the bacteriologic analysis of IS for the diagnosis of PTB in patients unable to expectorate sputum. The value of the clinical and HRCT characteristics in predicting IS culture positivity in these patients was also assessed.
Materials and Methods
1. Subjects
Medical records of the patients who underwent IS for the diagnosis of PTB between January 2011 and March 2014 at a tertiary university-affiliated hospital were reviewed retrospectively. Thirty-nine subjects who were unable to expectorate sputum spontaneously and finally diagnosed as PTB were included in this study. Exclusion criteria for the study were (1) patients who can produce sputum spontaneously, (2) patients who were on anti-tuberculosis treatment at the time of IS, and (3) age under 19 years. This study was approved by the Institutional Review Board.
2. IS procedure
IS was performed in the sputum induction room, equipped with a negative air-flow extraction fan that operated during the entire procedure. IS procedure was supervised by a trained nurse with standardized IS protocol. In order to minimize bronchoconstrictive response to saline inhalation, all subjects were premedicated with 200 µg salbutamol via metered-dose inhaler before sputum induction12. Sputum was induced through inhalation of 3% saline produced by an ultrasonic nebulizer OMRON NE-U17 (Omron Electronics, Seoul, Korea) for 15 minutes, and patients were encouraged to cough up and expectorate sputum into a sterile sputum pot at any time during and after the procedure.
3. Diagnosis of PTB
All IS specimens were subjected to AFB staining with auramine-O, and positive smears were confirmed with Ziehl-Neelsen staining. IS specimens were also subjected to mycobacterial culture on solid (Ogawa medium) and liquid medium (BACTEC MGIT 960 TB System; BD Biosciences, Sparks, MD, USA). Some IS specimens were also subjected to polymerase chain reaction (PCR) to detect target genes of M. tuberculosis (TB-PCR) (LG Life Science, Seoul, Korea). Further diagnostic studies like bronchoscopy with bronchoalveolar lavage (BAL), percutaneous needle biopsy (PCNB) and HRCT were analyzed. Final diagnosis of PTB was accepted when (1) M. tuberculosis was cultured or (2) there were evidences for presumptive diagnosis of PTB based on clinical, histological and radiological findings and appropriate response to anti-tuberculosis therapy.
4. Clinical and HRCT characteristics associated with IS culture positivity
Demographics (age and gender) and presence of specific clinical characteristics, such as symptoms (cough, fever, chest pain, and dyspnea), current smoking and previous PTB history were assessed. The presence of comorbid disorders and peripheral blood white blood cell counts were also assessed. Chest HRCT images were reviewed and the presence of characteristic features of PTB were assessed: (1) cavity, (2) centrilobular nodules, (3) tree-in-bud appearance (centrilobular nodules with linear branching opacities and clubbing of the distal bronchiole), (4) consolidation (opacities occluded air bronchogram >10 mm), and (5) miliary nodules1013. Clinical and HRCT characteristics that might be associated with IS culture positivity were evaluated by univariate and multivariate logistic regression analyses.
5. Statistical analysis
Data were analyzed using the statistical package SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). To assess the predictive value of clinical and HRCT characteristics for IS culture positivity, patients were divided into two groups based on positive and negative culture results of IS specimens. Logistic regression analysis was used to assess the univariate odds ratio and 95% confidence intervals of selected clinical and HRCT characteristics with culture positivity. Clinical and HRCT characteristics associated with culture positivity on a univariate analysis with p<0.20 were introduced into a multivariate analysis. p-values less than 0.05 were considered statistically significant.
Results
1. Characteristics of patients
Thirty-nine PTB patients who underwent IS due to absence of spontaneous sputum production were included in this study. Two patients were accompanied with tuberculous cervical lymphadenitis and four patients with tuberculous pleurisy. The clinical characteristics of the PTB patients are shown in Table 1. The mean age was 45.2±19.8 years (mean±SD). Nineteen (48.7%) were male and 20 (51.3%) were female. Eleven patients (28.3%) were current smokers and six (15.4%) had previous PTB history. Seven patients (17.9%) were accompanied with comorbid disorders: diabetes mellitus (n=4), chronic renal failure (n=1), Behcet's disease (n=1), and rheumatoid arthritis (n=1). Cough was the most common symptom found in 20 patients (51.3%) followed by chest pain in seven (17.9%), fever in three (7.7%), and dyspnea in one (2.6%). Twelve patients (30.8%) had no subjective symptoms and were identified through radiologic screening as a part of routine health check-up.

Clinical and HRCT characteristics of PTB patients (n=39)
2. Diagnosis of PTB
Seven of 39 IS specimens (17.9%) from PTB patients were AFB smear positive and 31 IS specimens (79.5%) were M. tuberculosis culture positive. All of the smear positive specimens were culture positive (Table 2). Of the eight subjects who were IS culture negative, one subject was confirmed PTB by bronchoscopy and BAL (M. tuberculosis culture positive). Seven M. tuberculosis culture negative patients both on IS and bronchoscopy) were clinically diagnosed as PTB based on clinical, histological and radiological findings and appropriate response to anti-tuberculosis therapy.
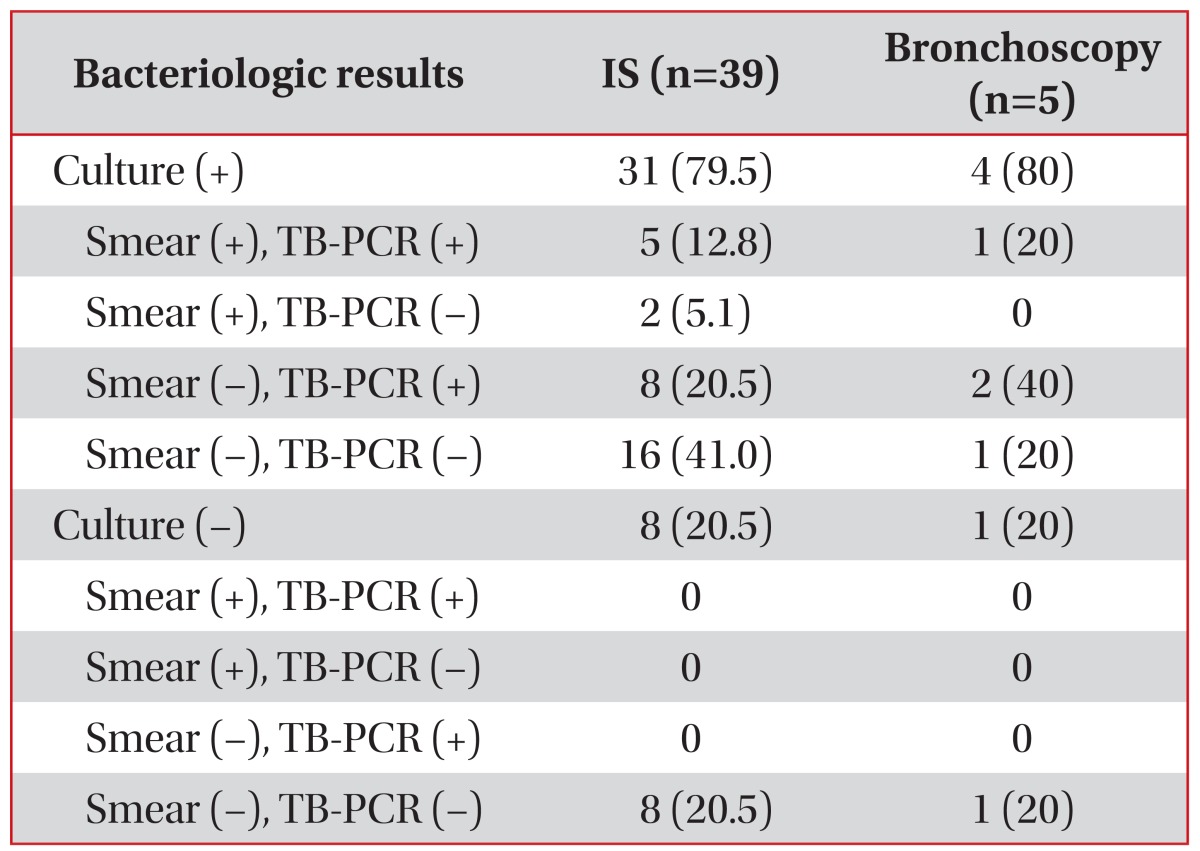
Bacteriologic study of IS (n=39) and bronchoscopy (n=5)
Twenty-four IS specimens were tested for TB-PCR and 13 (54.2%) were positive. All of the TB-PCR positive specimens were also positive on culture (Table 2). However, of the three IS specimens that were culture negative, none was TB-PCR positive. Eight of 24 smear negative specimens (33.3%) were positive on TB-PCR. Considering AFB smear and TB-PCR as early diagnostic methods, early diagnosis of PTB was possible with IS in 15 patients (38.5%). Of the 24 patients who failed early diagnosis with IS, 22 (91.7%) underwent HRCT, five (20.8%) underwent bronchoscopy with BAL, and four (16.7%) underwent PCNB of lung lesions. Of the five BAL specimens from bronchoscopy, four were positive on culture, one was positive on smear, and three were positive on TB-PCR (Table 2). Of the four PTB patients who were BAL culture positive, three were also IS culture positive. Thus, addition of bronchoscopy enabled bacteriologic diagnosis of PTB possible in 20% (1 of 5) and early diagnosis of PTB possible in 60% (3 of 5). Four PCNB specimens showed pathological findings suggesting tuberculosis (granulomatous inflammation with or without caseation necrosis or TB-PCR positive).
3. HRCT findings of PTB
Characteristic HRCT findings of 37 PTB patients are presented in Table 1. Centrilobular nodules (n=33, 89.2%) and tree-in bud appearance (n=24, 64.9%) were the most common HRCT findings seen in PTB. Consolidations were found in 10 patients (27.0%), cavities in two (5.4%), and miliary nodules in one (2.7%) (Table 1).
4. Clinical and HRCT characteristics associated with IS culture positivity
Among the 39 PTB patients, 31 patients (79.5%) showed IS culture positivity. Table 3 shows the results of univariate regression analysis of clinical characteristics associated with IS culture positivity. IS culture positive patients were younger than culture negative patients (p=0.07) and presence of cough was more frequent in the IS culture positive patients (p=0.11). Six patients who had previous PTB history were all IS culture positive and excluded from the analysis. Table 4 shows the results of univariate analysis of HRCT characteristics associated with IS culture positivity. The presence of tree-in-bud appearance (p=0.02) and centrilobular nodues (p=0.17) were more frequent in the IS culture positive patients. Two patients who had cavity on HRCT were all IS culture positive and excluded from the analysis. Multivariate analysis showed that younger age (p=0.04) and presence of tree-in-bud appearance on HRCT (p=0.03) were statistically significant independent predictors of IS culture positivity (Table 5).
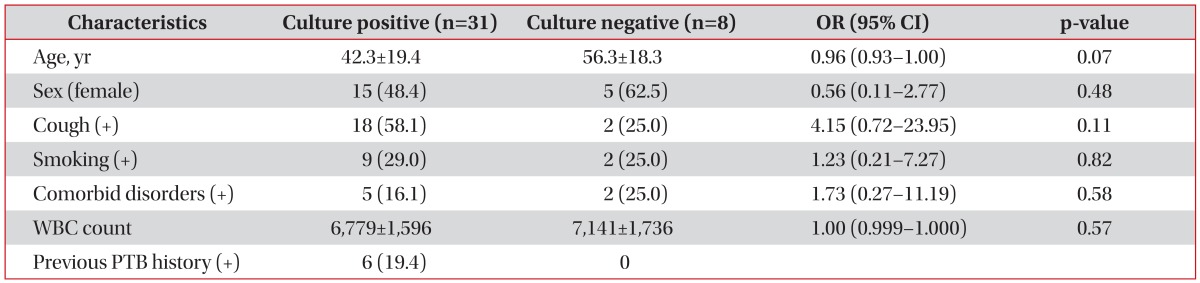
Univariate regression analysis of clinical characteristics associated with IS culture positivity (n=39)

Univariate regression analysis of HRCT characteristics associated with IS culture positivity (n=37)
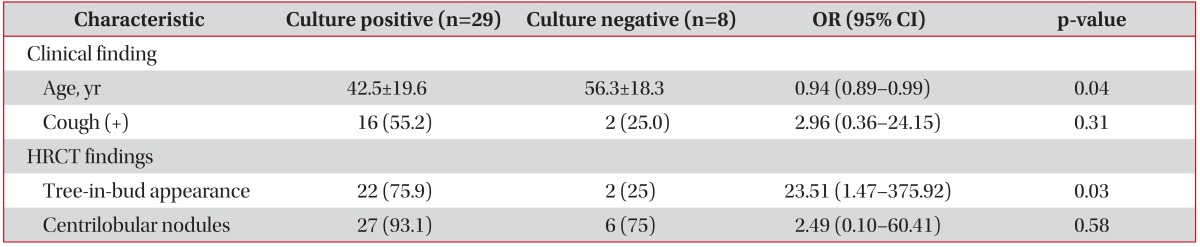
Multivariate regression analysis of clinical and radiological characteristics associated with IS culture positivity (n=37)
Discussion
IS through hypertonic saline inhalation has been shown to improve the diagnostic yield of PTB in patients with sputum smear negative or no reliable sputum production3414. However, a few studies in developed countries showed that the efficacy of IS is limited and adds little to the overall diagnosis yield of PTB67. In this study, IS culture was positive in 79.5% of patients unable to expectorate sputum, which is similar to other studies34. This study reconfirms that IS is useful for the diagnosis of PTB in clinical practice.
Sputum smears are positive in 22%-50% of patients with PTB15. However, this study showed that only in 17.9% of IS specimens from PTB patients unable to expectorate sputum were smear positive. Anderson et al.3 also reported that IS from sputum smear negative PTB patients shows low sensitivity for smear compared to culture (19% and 73%, respectively). Considering that smear examination requires at least 104 bacilli per milliliter to be positive, while culture can detect as few as 10-100 bacilli per milliliter, the low smear positive rate in the present study reflects the pauci-bacillary nature of IS specimens from PTB patients unable to expectorate sputum16.
Low sensitivity of sputum smear in the diagnosis of PTB is a common clinical problem leading to delays in the establishment of a diagnosis, because culture needs up to 8 weeks for sure results. The delay in diagnosis of PTB delays the isolation and treatment of patients, increasing the chance for spread of infection and the severity of the disease.
The development of TB-PCR has reduced the time required for the identification of the M. tuberculosis. Furthermore, sputum TB-PCR is more sensitive than AFB smear for the diagnosis of PTB1718. In this study, 33.3% of smear negative IS specimens were positive on TB-PCR while none of the culture negative IS specimens were positive on TB-PCR (Table 2). Kawada et al.19 showed that 56% of smear negative IS specimens were positive on TB-PCR and only 8% of culture negative IS specimens were positive on TB-PCR. These findings show that addition of TB-PCR to the bacteriologic study of IS specimens increases the chance of early diagnosis of PTB, but does not increase the final diagnosis rate of PTB significantly.
Recently, the recovery rate of nontuberculous mycobacteria (NTM) from respiratory specimens has increased in the South Korean population20. TB-PCR can discriminate between M. tuberculosis from NTM in smear positive specimens. Thus, the addition of TB-PCR to the bacteriologic study of IS should be recommended because it increases early diagnostic yields of PTB and allows exclusion of NTM if smear is positive.
Clinicians often face a dilemma when a patient suspected with PTB have negative IS smear and TB-PCR. They have a choice to either proceed with empirical treatment of PTB based on clinical and radiological findings, or to perform more invasive tests like bronchoscopy or PCNB to confirm the diagnosis3513.
In this study, only 37.5% of PTB patients (9 of 24) who failed to diagnose PTB early, were submitted to bronchoscopy or PCNB, while most (91.7%, 22 of 24) were submitted to HRCT. This might reflect that the attending physicians preferred to reach the presumptive diagnose of PTB based on radiological findings and start empirical therapy rather than performing more invasive procedures. Garcia et al.21 also reported that only 32% of IS smear negative patients were submitted to bronchoscopy for the confirmation of the diagnosis in clinical practice.
Several studies have reported that HRCT is superior to chest X-ray in the diagnosis of PTB1022. In one study, centrilobular nodules, tree-in-bud appearance, and cavity was detected in 91%, 71%, and 50% of PTB patients, respectively10. A few studies have reported the HRCT findings of smear negative PTB and showed that tree-in-bud appearance and centrilobular nodules were positively associated with PTB2324. However, HRCT findings in PTB patients unable to expectorate sputum have not been thoroughly investigated previously. In this study, centrilobular nodules and tree-in-bud appearance were detected on HRCT in 89.2% and 64.9% of PTB patients unable to expectorate sputum (Table 1). Cavity, the typical finding of PTB, is present in about 50% of PTB patients10. However, cavity formation is rarely observed in sputum smear-negative cases reflecting the smaller burden of mycobacterium11. This study also showed that cavity on HRCT was found only 5.4% of PTB patients unable to expectorate sputum. Cavity formation resulting from liquefaction and evacuation of caseous materials via the bronchi is a common cause of cough and sputum in tuberculosis. The low incidence of cavity in this study population may reflect the absence of spontaneous sputum production. Lee et al.23 reported that the sensitivity and specificity of HRCT for the diagnosis of PTB in sputum smear negative PTB suspects were 80.0% and 70.5%, respectively. These findings show that HRCT is also helpful for the diagnosis of PTB in patients unable to expectorate sputum. However, it should be kept in mind that the usefulness of HRCT in the diagnosis of PTB is limited especially in sputum smear negative cases25.
Garcia et al.21 showed that performing bronchoscopy after IS when smear results are negative increased the diagnostic yield of PTB by 64.1%. Although, only five of 24 patients (20.8%) who failed early diagnosis with IS underwent bronchoscopy in this study, the addition of bronchoscopy enabled early diagnosis of PTB in 60% (3 of 5) and increased bacteriologically confirmed diagnosis rate in 20% (1 of 5) (Table 2). Iyer et al.26 also showed that bronchoscopy provided diagnostic confirmation of PTB in 10% of patients suspected with PTB with negative IS smear and TB-PCR results. Thus, bronchoscopy may be useful for a rapid and accurate diagnosis of PTB when IS smear and TB-PCR are negative.
Culture for M. tuberculosis from respiratory specimen, standard diagnostic method of PTB, takes several weeks to get results. This study assessed the value of the clinical and HRCT characteristics in predicting IS culture positivity. Among the clinical characteristics, younger age was a statistically significant predictor of IS culture positivity (Table 5). Elderly patients have difficulty in producing sputum specimens despite hypertonic saline inhalation due to weakness and poor cooperation to the sputum inducing procedure compared to younger patients27. Thus, younger patients might have produced more adequate sputum specimen than elderly patients, reflecting higher IS culture positivity in younger patients in this study. Among HRCT findings, tree-in-bud appearance was also a statistically significant predictor of IS culture positivity. Feng et al.13 also reported that tree-in-bud appearance on computed tomography was independent predictor of PTB. Considering that tree-in-bud appearance reflects endobronchial spread of the disease, IS specimens from patients with tree-in-bud appearance on HRCT might have increased chances for obtaining sputum specimens including bacteria (Table 5)28. The presence of comorbid disorders was not associated with the IS culture positivity in this study, while immunocompromised patients are known to be susceptible to tuberculosis (Table 3). This might be due to limited number of cases for statistical analysis and absence of severe immunocompromised patients like acquired immunodeficiency syndrome.
This study has several limitations because it was retrospective in nature, using limited number of cases from available records, and the variables used in this study lacked uniformity. However, this study support the concept that IS is an effective method for the initial approach to patients with suspected pulmonary TB who are unable to produce sputum in clinical practice.
Acknowledgements
The present research was conducted by the research fund of Dankook University in 2013.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.