



Introduction
Real-time convex probe endobronchial ultrasound‒guided transbronchial needle aspiration (EBUS-TBNA) has become the standard of care for evaluating mediastinal and hilar lymphadenopathy [1]. Although EBUS-TBNA is a minimally invasive procedure with a high diagnostic yield, serious infectious complications such as mediastinitis, pericarditis, and sepsis have been reported [2-7]. Although rare, infectious complications can be life-threatening. We previously reported two cases of acute bacterial pericarditis after EBUS-TBNA, with one resulting in mortality [8].
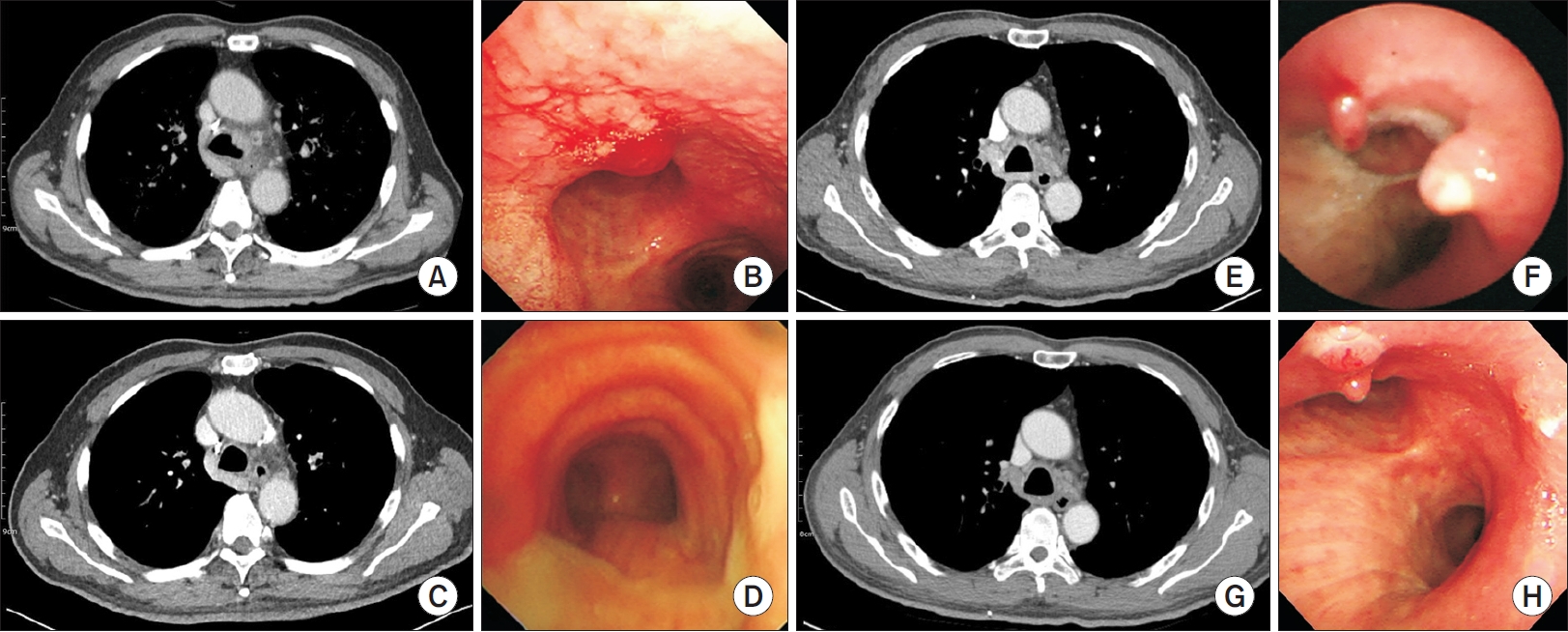
Recently our institution, a large tertiary referral hospital in South Korea, experienced two cases of mediastinal adenitis in patients with resectable lung cancer after EBUS-TBNA for mediastinal staging, which were initially misunderstood as lymph node metastasis on enhanced chest computed tomography scans (Figure 1). Although mediastinal adenitis was successfully managed by conservative treatment only, escalation of care was inevitable: prolonged hospital length of stay and operation time due to the presence of adhesions in the hilum in a patient with non-small cell lung cancer (Figure 1A-D), and prolonged hospital length of stay and a change in the treatment plan from surgery to chemoradiotherapy in the other patient with small cell lung cancer (Figure 1E-H).
Despite the occurrence of serious infectious complications after EBUS-TBNA, no consensus on any preventive strategies, including the use of prophylactic antibiotics, is available. Previous studies have suggested that the possible mechanism of infectious complications after EBUS-TBNA is the inoculation of oropharyngeal commensal bacteria into a target lesion by an aspiration needle [9-11]. When an EBUS bronchoscope passes through the oropharyngeal airway, the working channel of the scope can be contaminated by oropharyngeal commensal bacteria [7]. Therefore, an aspiration needle inserted through this channel can also be contaminated.
We assume that oral hygiene care is important in preventing infectious complications during EBUS-TBNA. Chlorhexidine gluconate is a broad-spectrum antimicrobial agent, and chlorhexidine gluconate mouthrinse is simple, safe, and widely practiced [12]. The aim of the present study is to investigate the effect of chlorhexidine mouthrinse on the prevention of microbial contamination during EBUS-TBNA.
Materials and Methods
1. Study design and setting
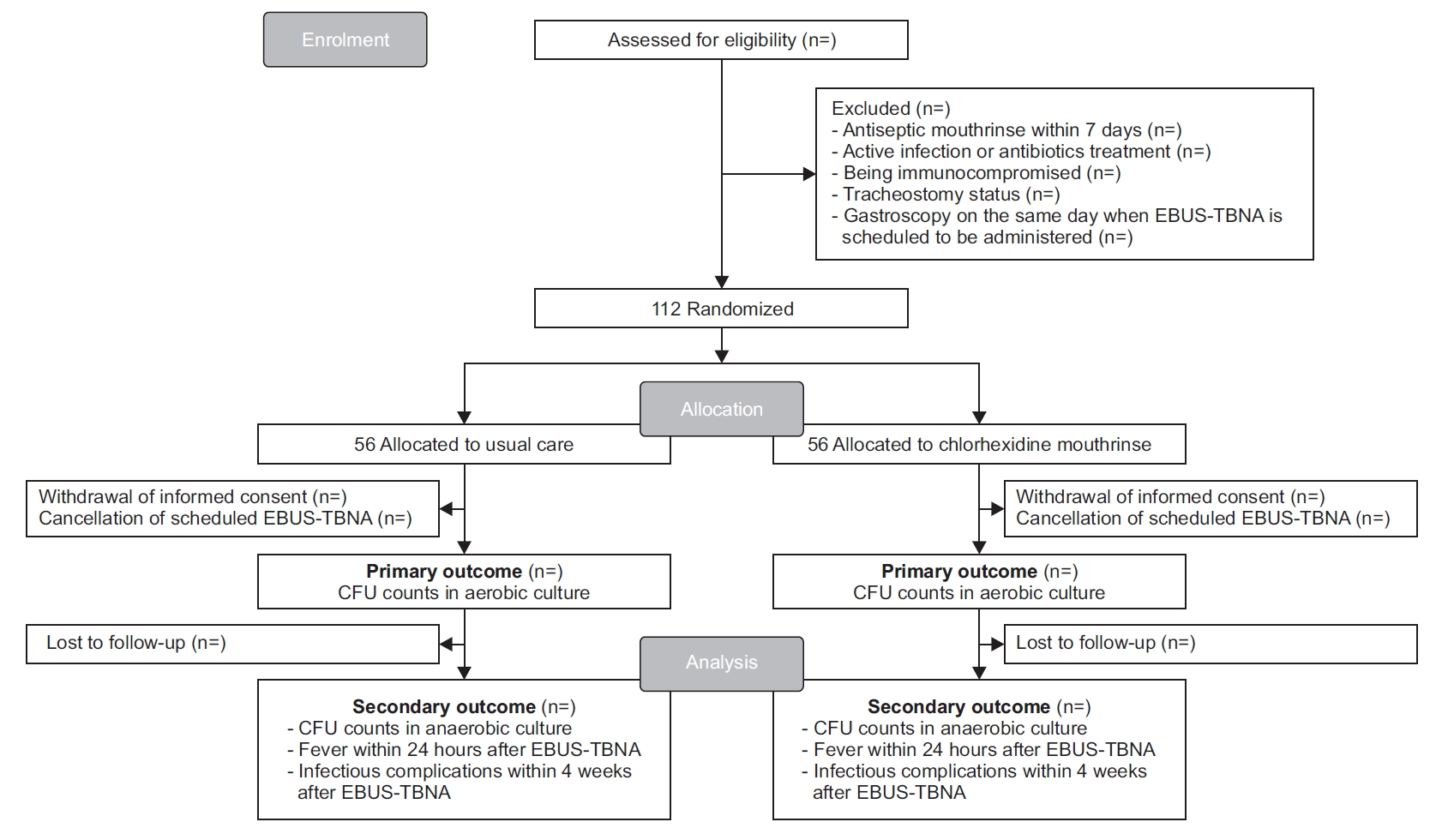
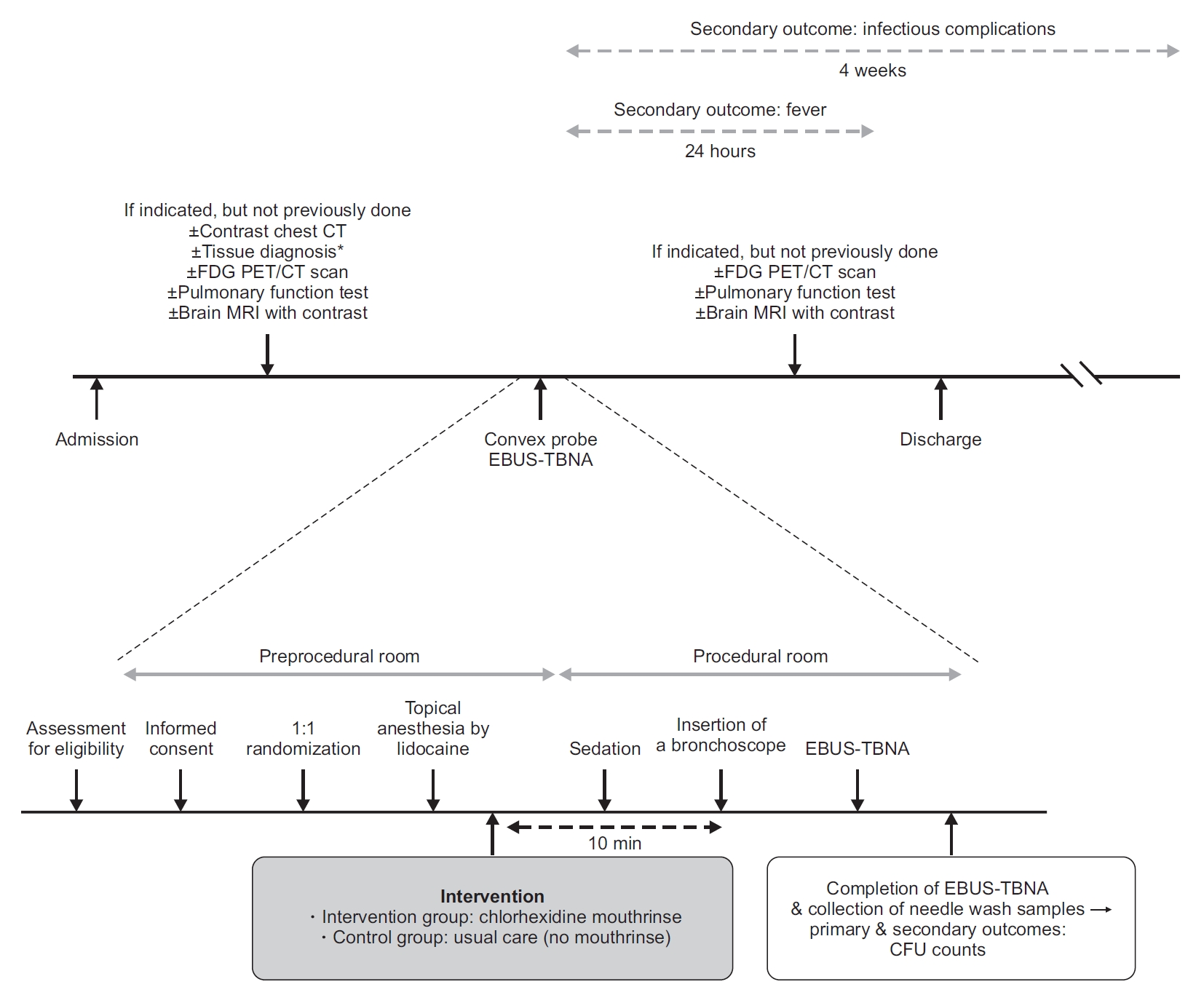
This study is a single-center, parallel-group, assessor-blinded randomized controlled trial (RCT) to be conducted at the Seoul National University Hospital in South Korea. Consenting and eligible participants who are scheduled to undergo EBUS-TBNA will be randomly assigned to either the intervention group or the control group at a 1:1 ratio. The flow diagram of this trial is shown in Figure 2. The protocol of this trial is described in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines [13] (Figure 3).
2. Eligibility criteria
Hospitalized patients aged 19 years and older who are scheduled to undergo EBUS-TBNA using a convex probe will be included in this trial. Patients will be excluded if they meet any of the following criteria: (1) antiseptic mouthrinse within 7 days before inclusion; (2) active infection or antibiotic treatment within 7 days before inclusion; (3) being immunocompromised status; or (4) tracheostomy status. We will also exclude patients who have already undergone gastroscopy on the same day when EBUS-TBNA is scheduled to be administered.
3. Topical anesthesia
Our dedicated bronchoscopy suite is composed of a preprocedural room, two procedural rooms, and a disinfection and reprocessing room. The postprocedural area is the same as the preprocedural room. In the preprocedural room, all patients will gargle with 20 mL of 1% lidocaine for topical oropharyngeal anesthesia (Figure 4).
4. Interventions
Following topical oropharyngeal anesthesia, participants who are assigned to the intervention group will gargle for 1 minute with 100 mL of 0.12% chlorhexidine gluconate in the preprocedural room. Participants in the control group will not be provided with mouthrinse. The chlorhexidine mouthrinse intervention will be performed approximately 10 minutes before insertion of the bronchoscope (Figure 4).
5. Implementation of EBUS-TBNA
After participants move to a procedural room, conscious sedation will be initiated with intravenous midazolam and adjuvant fentanyl administered by an experienced nurse and titrated by the attending bronchoscopist. As the flexible bronchoscope is advanced orally, 1% lidocaine solution will be used for “spray-as-you-go” administration to the trachea. Prior to EBUS-TBNA, an endobronchial examination of the bronchial trees will be routinely performed using a flexible bronchoscope (BF-1T260, BF-Q290, BF-260, BF-P260F, Olympus, Tokyo, Japan) unless it has been performed within the previous several days. During the procedure, basic diagnostic sampling methods (bronchial wash, bronchoalveolar lavage, bronchial brush, transbronchial lung biopsy, and endobronchial biopsy) can be performed at the bronchoscopist’s discretion. For EBUS-TBNA, an EBUS bronchoscope with a convex probe (BF-UC260FW, Olympus) will be inserted orally into the airway. Following identification of mediastinal or hilar lymph nodes by ultrasound, a 22-gauge aspiration needle (NA-201SX-4022 or NA-U401SX-4022, Olympus) will be advanced through the working channel of the bronchoscope to puncture the airway wall at the predetermined position. Paratracheal and peribronchial lung masses can also be sampled. The bronchoscopist can replace the aspiration needle with a new one during the procedure. Transesophageal bronchoscopic ultrasound-guided fine needle aspiration (EUS-B-FNA) will be allowed. For EUS-B-FNA, the same EBUS bronchoscope will be re-inserted into the esophagus after the completion of EBUS-TBNA. A 22-gauge aspiration needle (NA-201SX-4022 or NA-U401SX-4022, Olympus) will be used for sampling through the esophageal wall (either the same needle used in EBUS-TBNA or a new one). The NA-201SX-4022 is usually used during the procedure; however, the U401SX-4022 can also be used, especially when the supply of NA-201SX-4022 from the manufacturer is insufficient. All bronchoscopic procedures including EBUS-TBNA will be performed by an experienced pulmonologist or a fellow in pulmonary and critical care medicine under the close supervision of the pulmonologist. As part of standard care, patients will be monitored by an experienced nurse under the direction of the bronchoscopist. Prescription of prophylactic antibiotics after EBUS-TBNA is allowed, and its use, type, dosage, and duration will be determined by the bronchoscopist or care provider.
6. Microbial sample collection
Immediately after completion of EBUS-TBNA on all targeted lesions with an aspiration needle and ejection of all aspirated materials from the needle for pathologic evaluation, a needle wash sample will be taken by instilling 5 mL of sterile physiological saline solution into the used needle, and collecting it in a sterile 10 mL test tube. This collection method has been reported previously [10,14]. If the bronchoscopist uses two or more needles during the procedure, each needle wash sample will be collected in each sterile tube immediately after completing the procedure. The samples will be immediately refrigerated at 5°C and processed on the same day.
Bacterial culture of the needle wash samples will be performed according to a routine clinical protocol. Needle wash samples will be plated on blood agar and chocolate agar plates, and incubated for 2 days under aerobic conditions. The samples will also be plated on Brucella agar plates, and incubated for 2-4 days under anaerobic conditions. If two or more needles are used per participant, each needle wash sample will be plated and incubated under both aerobic and anaerobic conditions. The bacteria will be identified by matrix-assisted laser desorption ionization (MALDI) time-of-flight mass spectrometry using a microflex LT (Bruker Daltonics, Bremen, Germany). A colony will be placed on the target plate by the direct transfer method and analyzed with MALDI Biotyper RTC software 3.1 and the BDAL database (6903 MSP). A colony forming unit (CFU) will be measured according to the colony morphology and the result of identification.
7. Outcomes
The primary outcome is CFU counts in aerobic culture. If two or more needle wash samples are obtained in a participant, the primary outcome is the average of CFU counts in the aerobic plates. Secondary outcomes include CFU counts in anaerobic culture, fever within 24 hours after EBUS-TBNA, and infectious complications within 4 weeks after EBUS-TBNA. If two or more needle wash samples are obtained in a participant, the average of CFU counts in the anaerobic cultures will be used as a secondary outcome measure. Fever is defined as a temperature ≥37.8°C. Infectious complications include pneumonia, lung abscess, empyema, mediastinal adenitis/abscess, mediastinitis, pericarditis, and sepsis.
8. Estimated sample size
Sample size calculations are based on an available RCT of 100 patients who underwent gastroscopy with or without chlorhexidine mouthrinse due to a lack of similar previous studies on EBUS-TBNA [15]. To test whether chlorhexidine mouthrinse reduces the CFU counts of needle wash samples by 50% with a power of 90% and an alpha of 0.05, the required sample size per group is 50. Considering a potential dropout rate of 10%, a sample size of 56 per group (112 in total) is required.
9. Randomization
A web-based randomization system has been implemented by the Medical Research Collaborating Center of the Seoul National University Hospital (https://mrcc.snuh.org/). A clinical research coordinator will perform randomization through the website. Each patient will be assigned an alphanumeric code. Investigators and other research personnel are unable to access the website. Only the clinical research coordinator is able to view intervention allocation on the website.
10. Blinding
The following personnel will be blinded to the intervention assignment: investigators including bronchoscopists performing EBUS-TBNA, technicians assisting with the procedure and instilling saline into aspiration needles to collect needle wash samples, outcome assessors including laboratory personnel, and care providers in general wards. Mouthrinsing with chlorhexidine will be done in the preprocedural room, which is separate from the procedural room, and bronchoscopists and assisting technicians in the procedural room can be blinded. However, participants are not blinded to the intervention assignment. Participants in the control group receive usual care (no mouthrinse). A placebo control such as pure water with or without a flavored additive will not be used in this trial because participants will be able to distinguish between chlorhexidine and placebos due to the odor and taste of chlorhexidine. Unblinding to an attending bronchoscopist performing EBUS-TBNA is possible if serious adverse events such as shock or seizure occur and if a relationship between the events and the chlorhexidine mouthrinse is suspected by the attending bronchoscopist. However, this unblinding has no consequence on the primary outcome measure.
11. Data collection
The below data will be collected.
1) Patient factors
(1) Demographic information: age, sex, body mass index, and smoking status
(2) The purpose for EBUS-TBNA: diagnosis and staging of malignancy or diagnosis of benign diseases such as tuberculous lymphadenitis and sarcoidosis
(3) Comorbidities: hypertension, diabetes mellitus, coronary heart disease, heart failure, stroke, chronic liver disease, chronic kidney disease, chronic obstructive pulmonary disease, and asthma
(4) Pathologic diagnosis
(5) Prescription of prophylactic antibiotics after EBUS-TBNA, and its type, dosage, and duration
2) Procedural factors
(1) Bronchoscopic procedures other than EBUS-TBNA: bronchial wash, bronchoalveolar lavage, bronchial brush, transbronchial lung biopsy, endobronchial biopsy, and EUS-B-FNA
(2) The number of insertions of the EBUS bronchoscope
(3) The total number of lymph nodes punctured and the number of needle punctures per lymph node
(4) The number of aspiration needles used
(5) Characteristics of lymph nodes: size (less or more than 1 cm), shape (oval or round), margin (indistinct or distinct), echogenicity (homogeneous or heterogeneous), and the presence of cyst, central hilar structure, coagulation necrosis sign, calcification, and pus-like discharge
(6) Procedure time, type and dosage of sedatives, attending bronchoscopists and their expertise
(7) Adverse events after chlorhexidine mouthrinse
12. Statistical analysis
In all analyses, patients will be analyzed according to their randomization groups, with the exception of those who withdraw informed consent or do not undergo scheduled EBUS-TBNA (e.g., cancellation of scheduled EBUS-TBNA after successful diagnostic procedures such as endobronchial biopsy). CFU counts in the aerobic and anaerobic cultures of needle wash samples will be expressed as the mean±standard deviation and analyzed by the independent samples t test if distributed normally. Otherwise, they will be described as the median (interquartile range) and analyzed using the Mann-Whitney U test. Fever within 24 hours after EBUS-TBNA and infectious complications within 4 weeks after the procedure will be presented as numbers and percentages and analyzed by either the chi-square test or Fisher exact test. Subgroup analysis according to the use of EUS-B-FNA and prophylactic antibiotics will be conducted. For the subgroup analysis according to prophylactic antibiotic use, only fever and infectious complications will be analyzed as outcomes. All comparisons will be two-sided and p-values of less than 0.05 will be considered statistically significant.
13. Research ethics approval
This study was approved by the Institutional Review Board of Seoul National University Hospital (H-2011-096-1173). This trial will be conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice. Written informed consent will be obtained from all participants before randomization.
14. Confidentiality
All data will be anonymized and identified by a coded ID number only to maintain participant confidentiality. All records containing personal identifiers such as informed consent forms will be stored separately from records identified by the coded ID number. All data will be stored in either a locked filing cabinet or in an electronic password-protected computer in a locked office. The access to data is restricted to authorized personnel only.
Discussion
EBUS-TBNA is a minimally invasive procedure; however, infectious complications following EBUS-TBNA can be fatal. To date, there have been limited data on preventive strategies to reduce infectious complications following EBUS-TBNA. We hypothesize that oral hygiene care has a role in preventing infectious complications after EBUS-TBNA.
Several studies have proposed that infectious complications after EBUS-TBNA are related to contamination of aspiration needles with oropharyngeal flora [4,9-11]. As the EBUS bronchoscope passes through the oral cavity and pharynx, the working channel of the scope can be contaminated by oropharyngeal flora. Microorganisms might be inoculated by puncture with the contaminated aspiration needle inserted through this channel. A previous study reported that contamination of aspiration needles with oropharyngeal commensal bacteria was relatively common—one-third of aspiration needle wash cultures were positive for typical oropharyngeal flora [14]. Moreover, a retrospective study showed that insertion of the EBUS bronchoscope through an endobronchial tube reduced contamination by oropharyngeal commensal bacteria—aspiration needle wash cultures were positive in only 3% of patients with endobronchial tubes, but in 100% of those without endobronchial tubes [10].
Chlorhexidine mouthrinse is a promising candidate to prevent infectious complications following EBUS-TBNA. First, chlorhexidine gluconate has a broad spectrum of antimicrobial activity against gram-positive and gram-negative bacteria as well as yeast [12]. Second, oral hygiene care with chlorhexidine is widely practiced in critical care medicine because it reduces the risk of developing ventilator-associated pneumonia [16]. Third, a previous RCT in patients undergoing gastroscopy demonstrated that chlorhexidine mouthrinse reduced microbial CFU counts by 88% in endoscope samples [15]. Fourth, chlorhexidine mouthrinse is simple, safe, and cost-effective.
There are several risk factors other than contamination of the working channel or aspiration needle for developing infectious complications after EBUS-TBNA: the number of needle punctures per lymph node; the total number of lymph nodes punctured; the characteristics of lymph nodes (necrotic or cystic); and the expertise of the bronchoscopist [7]. These data will be collected in this trial.
This study will have limitations. Sample size estimation might be imprecise because it was based on an RCT in patients who underwent gastroscopy with or without chlorhexidine mouthrinse [15]. In addition, the primary outcome is a surrogate measure for the risk of infectious complications of EBUS-TBNA. If this trial proves the effectiveness of chlorhexidine mouthrinse in preventing microbial contamination during EBUS-TBNA, further large-scale studies will be required to assess outcomes such as the incidence of infectious complications following this procedure.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






