



Introduction
By the end of December 2019, a new viral infection that mainly affects the human lower respiratory tract was first detected in China and quickly spread out to all over the world within a few weeks. This novel virus is type 2 severe acute respiratory syndrome coronavirus (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19) [1]. COVID-19 is a highly contagious disease that has rapidly spread worldwide and has been announced as a pandemic by the World Health Organization (WHO). More than 5.7 million individuals worldwide were infected, and approximately 358,000 death cases were reported by 28 May [2]. There are many factors that might cause the large variations in the prevalence and death rate of COVID-19 among countries. One of these factors is whether a country enacts vaccination prevention programs against serious infectious diseases, such as tuberculosis (TB). Although TB and COVID-19 are caused by two different microorganisms, both infect the lower respiratory tract and are transmitted via small respiratory droplets coughed or sneezed by an infected patient. In addition, any of these two diseases are known to be a deadly infection for people with weak immunity system. Epidemiological data on the global prevalence of COVID-19 indicated that countries with bacillus CalmetteGuérin (BCG) vaccination policies have lower rate of death related to COVID-19 than in countries without such a policy [3,4].
Vaccine for Mycobacterium tuberculosis and the Immune System
TB is caused by bacterial infection of Mycobacterium tuberculosis to the human body through mainly the pulmonary route. This Mycobacterium species is present in the air coughed by individuals with TB. The most common symptom is persistent cough. TB can affect the lymph nodes, which are essential for proper functioning of the immune system. Long-course (at least 6 months) treatment with antibiotics, such as rifampicin and ethambutol, can be used to completely cure TB [5].
BCG vaccine for TB is prepared from a weakened strain of Mycobacterium bovis. This bacterial strain is very close to M. tuberculosis, which causes TB in humans [6]. This BCG vaccine is typically administered shortly after birth to protect infants and children from serious forms of TB, particularly to prevent pulmonary TB. In brief, the immune response induced in newborns after BCG vaccination typically starts with the recognition of BCG by neutrophils, macrophages, and dendritic cells at the inoculation site. This is followed by the activation of the adaptive immune system via migration of dendritic cells to the lymph nodes, resulting in the activation of mycobacteriaspecific CD4 and CD8 T cells, which secrete high amounts of interferon (IFN)-γ and granzymes (serine proteases enzymes released within cytotoxic T cells and natural killer cells for inducing apoptosis to eliminate cells that have become cancerous or infected with bacteria or viruses). This subsequently leads to the activation of B cells and the generation of plasma and memory T cells in addition to the production of antigenspecific antibodies in response to the presence of BCG antigens. These antibodies help protect the body against TB infection. Some evidence also shows that BCG vaccine induces non-specific cross-protection via improved innate immune responses against microorganisms other than the TB-related pathogen [7,8]. Recently, it was found that inf-cDC2s, a type of dendritic cells, play an important role in body responses to SARS-CoV-2 infection in vivo, as these cells are generated in a type I IFN-dependent manner to optimally prime CD4+ and CD8+ T cell immunity and to induce much stronger immune responses [9]. Moreover, BCG vaccine is associated with low hospitalization rates for other respiratory infections not related to TB [10].
Although national BCG vaccination programs are available in most countries apart from Western European countries and North American countries, such as the United States and Canada, TB remains a life-threatening disease with 1.5 million deaths in 2018 worldwide; moreover, it is estimated that 10 million people suffer from TB globally, with most cases occurring in eight countries: India, China, Indonesia, the Philippines, Pakistan, Nigeria, Bangladesh, and South Africa [11]. The main reason for that is the efficacy of BCG vaccine in preventing pulmonary TB by 50% in average [12,13]. This means that BCG vaccine can reduce the risk of TB and its progression to active TB. Likewise, COVID-19 death records in those countries were less than 6 per 1 million of population [2]. Yet, BCG vaccine does not provide complete protection against TB owing to many factors, such as genetic differences among the populations, environmental changes, exposure to specific strains of TB or other bacterial, and the TB strains used to manufacture the vaccine. These factors also include genetic differences between the strains being cultured and the choice of growth medium [14,15].
In addition, the duration of protection by BCG is not clearly known, as published data showed an inconsistent protective effect of the BCG vaccine [16-19]. One study found that in a given population, the protective effect of BCG against TB could decrease after 15 years and probably disappeared after 20 years [19], whereas another study in Native Americans immunized in the 1930s found evidence of protection even at 60 years after immunization, with only a slight waning in efficacy [20].
In 2018, 153 countries were considering the BCG vaccine as a standard childhood immunization program, and there are only 113 countries with a BCG coverage of ≥90% of the population [11].
Published Information about the Proposed Role of BCG in Activating the Immune System against COVID-19
The BCG vaccine typical enhances the immune system capability to fight off pathogens, by interacting immune cells receptors with different pathogen associated molecular patterns, such as peptidoglycans, cell wall proteins, lipopolysaccharides, mycolic acids and glycoproteins which locate at the pathogen cell membrane and preserve molecular signatures of bacteria and viruses as well [7,21]. Following this reaction, a series of biological stimulations take place including the production and secretion of pro-inflammatory cytokines as described in section 2. In particular, the BCG vaccine was found to be also defending against viral infections which affect the respiratory tract. In this context, it was found that mice who vaccinated with BCG prior to be infected with the Influenza virus have mild lung damage and lower Influenza load in their blood compared to those did not vaccinated and this was referred to either an earlier antibody secretion or the nonspecific cell-mediated immunity [22].
In an experimental laboratory setting, the BCG vaccination exhibited the capability to reduce the level of the yellow fever vaccine (an attenuated viral strain) viremia in human monocytes and this was correlated with induction of cytokine responses (especially interleukin [IL]-1b) [23].
In a randomized placebo-controlled pilot study, healthy volunteers received either placebo vaccine (n=20) or live attenuated BCG vaccine (n=20). After 14 days, all participants received intramuscular injection of trivalent influenza vaccine. Antibody responses against that influenza vaccine strain were significantly enhanced in BCG group compared to the placebo group. Enhanced pro-inflammatory leukocyte responses and modulation of cytokine responses against unrelated pathogens were observed [24].
Likewise, the BCG vaccine might probably induce such a mechanism in the human body against COVID-19 which could result in reducing both the COVID-19 death rate and the severity of cases.
COVID-19 Pandemic
COVID-19 was first reported in Wuhan City, Hubei Province, China in December 2019, and the disease spread rapidly in China and globally in less than 5 weeks [25]. Coronaviruses are a family of viruses that commonly exist in nature and can infect humans, causing pneumonia, kidney failure, damage in the digestive tracts, and even death [26]. Currently, the novel COVID-19 is spreading more quickly than other known coronaviruses [27].
COVID-19 is mainly transmitted between people via close contact or respiratory droplets coughed or sneezed by COVID-19-infected people. The high incidence of COVID-19 could probably be caused by the spreading of the virus via asymptomatic infected individuals. The initial site of COVID-19 infection is not yet defined, and its pathogenesis is still under investigation. Because COVID-19 is a respiratory disease, the lungs of most COVID-19 patients appear to be affected. The common symptoms of COVID-19 are fever, cough, fatigue, sore throat, and shortness of breath [27,28].
In severe COVID-19 cases, high levels of pro-inflammatory cytokines (IL-2, IL-7, IL-10, granulocyte colony-stimulating factor, IFN-γ-induced protein 10, monocyte chemotactic protein 1, macrophage inflammatory protein 1A, and tumor necrosis factor α), a phenomenon known as cytokine storm, were observed [25]. This cytokine storm can lead to inflammation-induced lung damage with serious complications, such as pneumonia, respiratory failure, shock, and even death [29]. Currently, paracetamol as an antipyretic/analgesic agent as well as empirical antibiotics for co-infections are common treatment options used to manage COVID-19 cases in hospitals worldwide [30].
Both the incidence and death rates of COVID-19 in the United States and most European countries (which should have robust healthcare systems) were higher than those in other developed countries with good healthcare systems, such as Singapore, Japan, Korea, and Hong Kong, and also higher than that in developing countries that might not have well-established healthcare systems [2].
Based on BCG data of the last 40 years published by WHO, countries with more than 10,000 confirmed COVID-19 cases were classified as BCG and non-BCG countries in this review article [31]. Till 28th of May 2020, the WHO data revealed that the incidence of COVID-19 (cases per 1 million of population) in countries with a national BCG vaccination policy is 3.6-fold lower than that in countries without such a policy, based on the medians of the two groups (Table 1). Regardless of the number of countries used in this comparison, the number of COVID-19 cases is also higher by two-fold in countries without a national BCG vaccination policy than in countries with such a policy, based on the medians of the two groups (Table 1).
In this context, another research group was found that the reported number of COVID-19 cases are very low in the countries with universal BCG vaccination policies compared to countries without such a policy [21].
BCG Vaccination and COVID-19 Death Occurrence
In general, the death rate of COVID-19 in each country is mainly related to the age and health conditions (such as cardiovascular diseases, diabetes, and weak immune system) of COVID-19 patients [32,33]. Moreover, the numbers of COVID-19 death cases varied among non-BCG countries (Table 1). For example, the number of COVID-19 death cases in Germany is 4.4-fold lower than that in the United Kingdom. This can be further expressed as one death case per 21 COVID-19 cases in Germany, whereas in the United Kingdom the number was one death case per seven COVID-19 cases. This might be attributed to the differences between Germany and the United Kingdom in terms of healthcare settings and actions taken by governments to minimize the spreading of COVID-19.
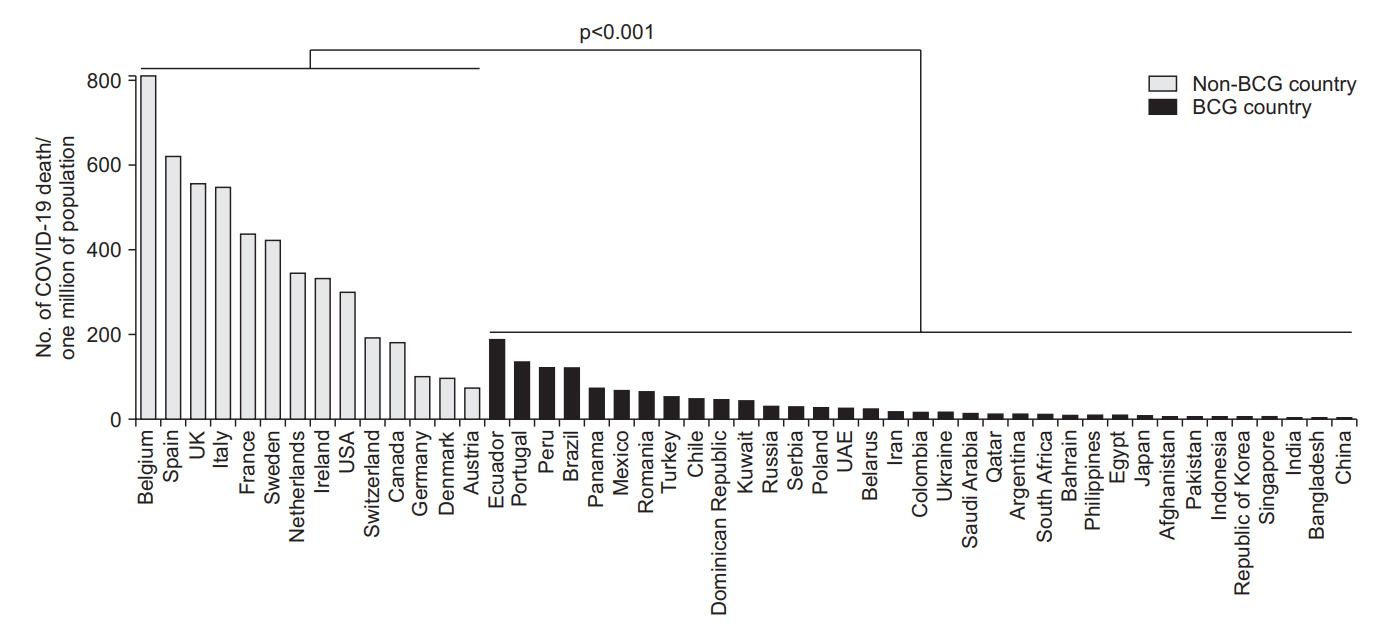
COVID-19 death cases (per 1 million of the population) in countries with more than 10,000 confirmed COVID-19 cases were also reviewed and reported (Table 1). The occurrence of COVID-19 death is 21-fold lower in countries with a national BCG vaccination policy than in countries without the policy, based on the medians of COVID-19 death case per 1 million of population in these two groups of countries (p<0.001, MannWhitney test). Moreover, the odds ratio for COVID-19 death in countries with BCG vaccination program was found to be 0.15 (95% confidence interval [CI], 0.14-0.16). In particular, the highest reported values of COVID-19 death case per 1 million of population in a non-BCG country and a BCG country were 810 (in Belgium) and 188 (in Ecuador), respectively (Table 1, Figure 1).
Moreover, a median of one death case per 10 cases of COVID-19 was reported in non-BCG countries, compared with one death case per 37 cases of COVID-19 in BCG countries. Furthermore, the number of COVID-19 death cases in BCG countries was nine times lower than that in non-BCG countries, based on the medians of COVID-19 death cases in these two groups of countries (Table 1).
However, the race, age, health conditions, and location of COVID-19 patients, as well as the number of population per country and actions taken by governments, might affect the occurrence of COVID-19 death. In particular, the presence of a national BCG vaccination policy appeared to have a great impact on reducing the rate of COVID-19 death in a given country. For example, the COVID-19 death case per 1 million of population in Spain (a non-BCG country) is 4.6- and 89- fold higher than that in Portugal and Japan (BCG countries), respectively (Table 1). This can also be further expressed as one death case per 23 in Portugal and per 19 in Japan (BCG countries), whereas in Spain (a non-BCG country) the number was one death case per eight cases of COVID-19. Furthermore, Japan and India had already established national BCG vaccination polices in 1951 and 1962, respectively, and experienced seven and three COVID-19 death cases per 1 million of population in 2020, respectively [34,35].
These findings were in line with those recently published by Hegarty’s team (2020), who generally reported a mean COVID-19 death rate of 4.28 per 1 million of population in countries with national BCG vaccination policies compared with 40 per 1 million of population in countries without such policies; they also indicated that a booster dose of BCG vaccine between 7 to 14 years after the first vaccination did not lead to better outcomes compared with single-dose vaccination [3]. In this context, Miller’s research team (2020) also found that the presence of established BCG vaccination policy correlated with a reduced COVID-19 death rate in a given country. However, this does not clearly prove that BCG vaccine would enhance defences in older adults [4]. Another research group was also indicated that the data in the literature can suggest a possible inverse correlation between BCG immunization and the number of COVID-19 cases and severity [36]. At the same time, it was recommended to do not use the BCG for preventing or managing COVID-19 with no direct evidence from clinical trials [37]. Therefore, several countries started clinical trials on the BCG vaccine as it could be a potential prophylactic treatment until producing the appropriate COVID-19 vaccine.
Variations in the number of COVID-19 death cases among countries without a national BCG vaccination policy can also be explained by their history of BCG vaccination coverage. For example, in Denmark, BCG vaccination was neither mandatory nor recommended from 1975; however, BCG vaccination was started in 1946 and was recommended until the early 1980s, and BCG vaccination coverage for children born in 1965 was 60% [38]. In Germany, according to the Robert Koch Institute’s national tally, BCG vaccination was more common in East Berlin than in West Berlin, covering 94.2% and 16.5% of the population, respectively [39]. In addition, 621 COVID-19 death cases per 1 million of population were reported in Spain, where BCG vaccination was introduced in 1965 and stopped in 1981. Finally, 134 COVID-19 death cases per 1 million of population were reported in Portugal, where a BCG vaccination program was also introduced in 1965 [27].
On the other side, there are debates about the association of the presence of active BCG vaccination programs with the COVID-19 related prevalence and mortality rate [40,41]. These studies actually denying any association between COVID-19 incidence rates and the presence of active BCG vaccination policies. But there is no disagreeing for a relation with the COVID-19 mortality rate as described in this review. However, BCG vaccination programs might be not a magical resolution for COVID-19, as there are many other factors, in addition to these programs need years to develop human protection immunity to reduce consequence of SARS-CoV-2 virus infections. This review highlights the possibility of the protective role of BCG in the context of COVID-19 which can also explain why there are 12 registered BCG-coronavirus clinical trials. Therefore, there is a real need to wait for the results of clinical trials.
Recent COVID-19 BCG-Related Clinical Trials
Many clinical trials are being conducted to determine whether BCG vaccine can reduce the frequency and severity of COVID-19 symptoms. Currently, there are 12 clinical trials in 12 countries, all of which are registered in the official website of clinical trials; these studies are aimed to evaluate the protective effect of BCG vaccine against COVID-19 in healthcare workers (Table 2) [42].
Conclusion
It can be concluded that the presence of a national BCG vaccination policy in a given country could potentially offer a beneficial protective effect against TB and other nonspecific infectious diseases. Likewise, BCG could be one of the reasons of low the number of COVID-19 death cases or lower the severity of COVID-19 cases in the same country as per the WHO data till 28th of May 2020. According to the records, the BCG vaccine might also play a role in decreasing the incidence of COVID-19 in countries with a BCG national vaccination program. However, the available WHO information on BCG vaccination policies in different countries covers only the last 40 years. In BCG countries, most COVID-19 death cases occurred in people aged ≥50 years, which indicate that BCG vaccine may offer indirect protection or herd immunity in these countries.
This review found that the probability of death due to COVID-19 could be lower in individuals born in countries that adopt BCG vaccination policy (i.e., individuals vaccinated with BCG shortly after birth) than in those born in countries without a BCG vaccination policy.
Finally, investigating into the effect of BCG vaccine on individuals with COVID-19 in the clinical trial setting might be a helpful approach to confirm whether BCG is effective in managing the current COVID-19 pandemic and the anticipated second wave of this infection in the coming winter. Meanwhile, these studies are needed, especially in the absence of a marked vaccine against COVID-19 and in the presence of records and reports which support the role of the BCG vaccine in activating the human immunity system against respiratory viral infections.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






